
Here are some selected slides and notes from this year’s NASPGHAN’s postrgraduate course. There may be some errors of omission or transcription.
Link to the full NASPGHAN PG Syllabus 2019 (Borrowed with permission)
Functional/Motility Session
95 Carlo Di Lorenzo, MD, Nationwide Children’s Hospital. Evaluation Testing for functional disorders: The indispensable, the useless, the dangerous and treatment strategies in NERD and functional dyspepsia.
This was the best lecture of the day!!! (Hence a lot of slides follow)
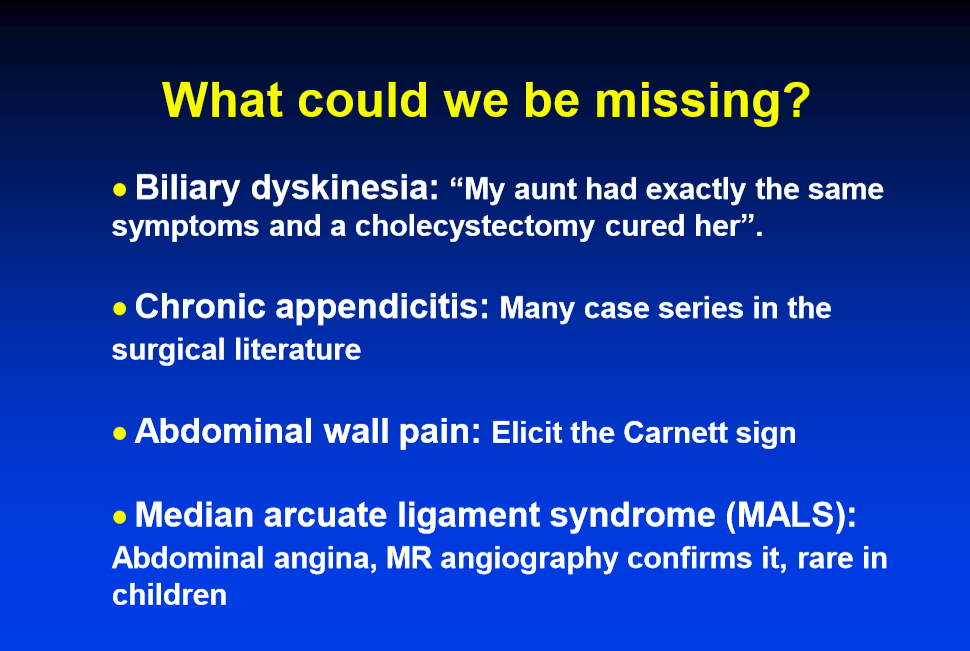
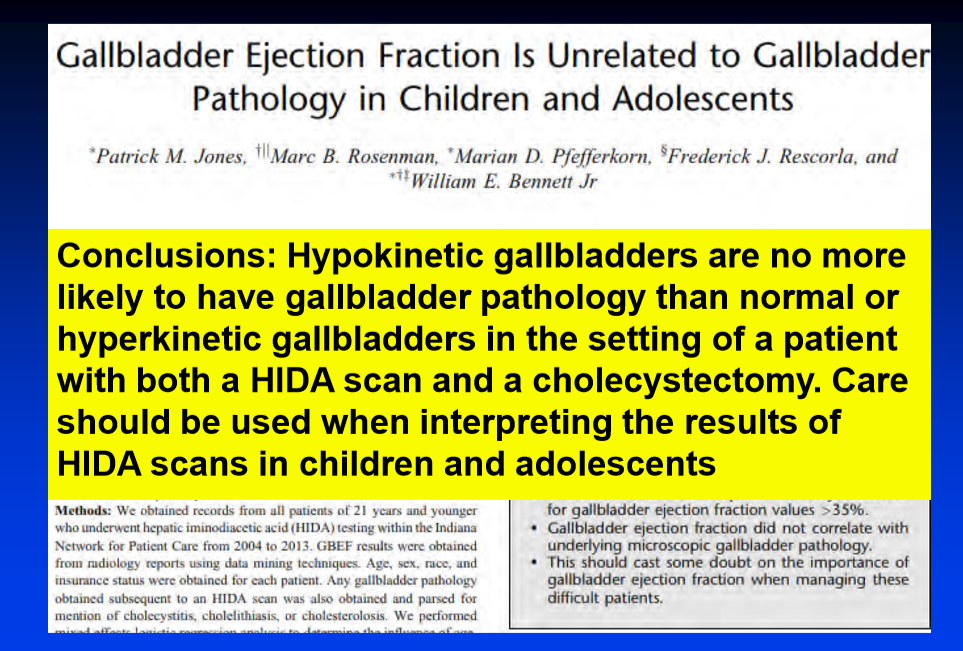
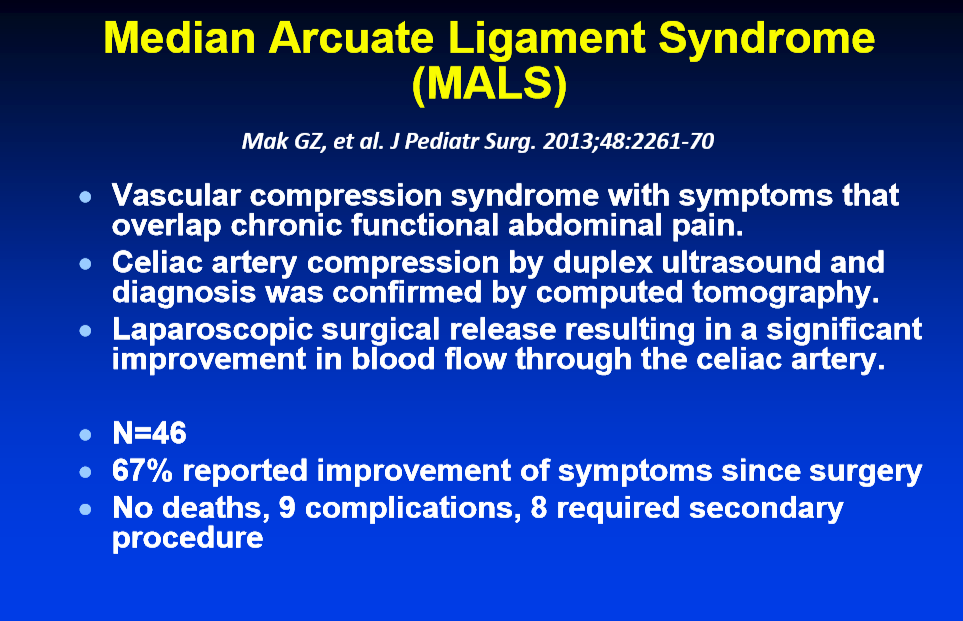
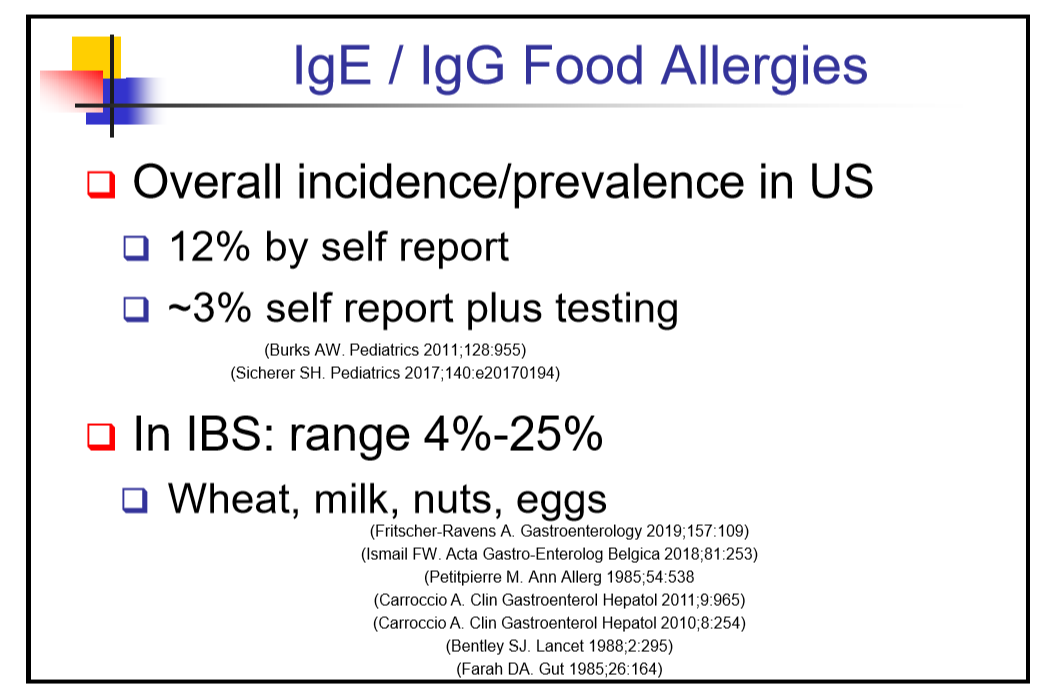
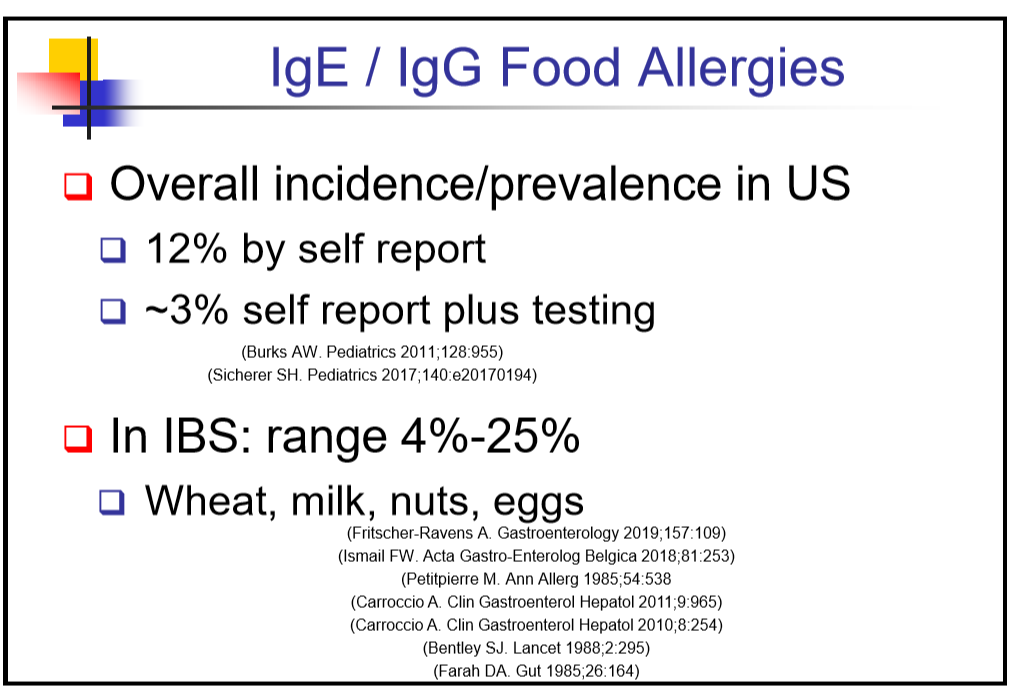
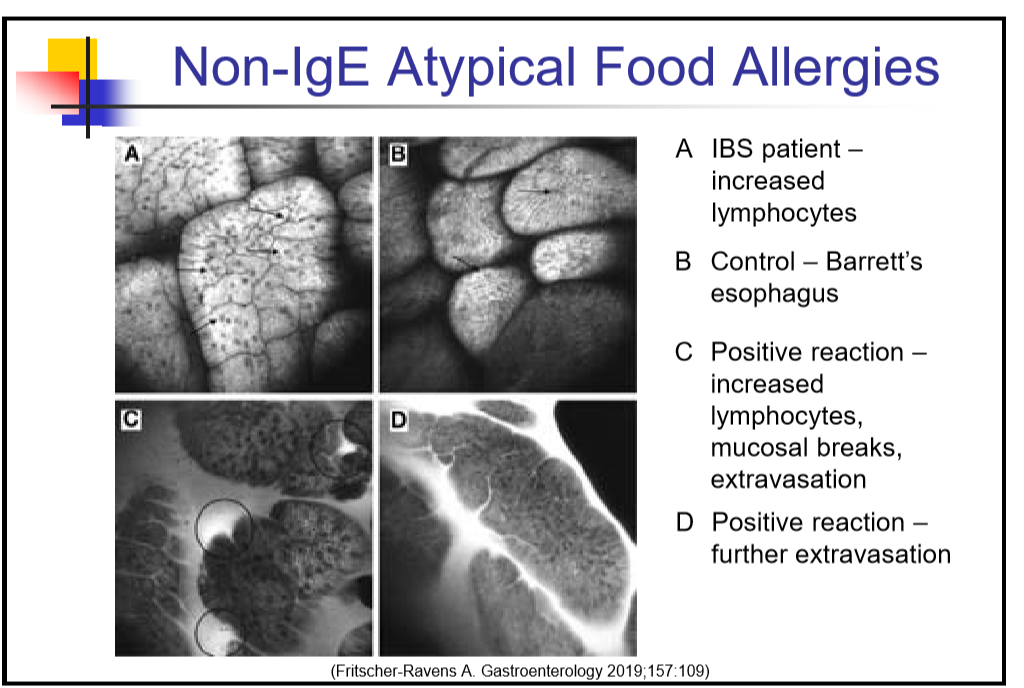
- Families never complain about doctors missing irritable bowel syndrome and anxiety. They may complain about missing diagnosis which are controversial with regarding to chronic pain (‘chronic appendicitis, gallbladder dyskinesia, ‘mild’ IBD, median arcuate ligament syndrome, and food allergies)
- Functional disorders, but not organic disorders, can cause ‘constant’ pain. “Tried everything.” Functional disorder patients frequently have side effects with everything.
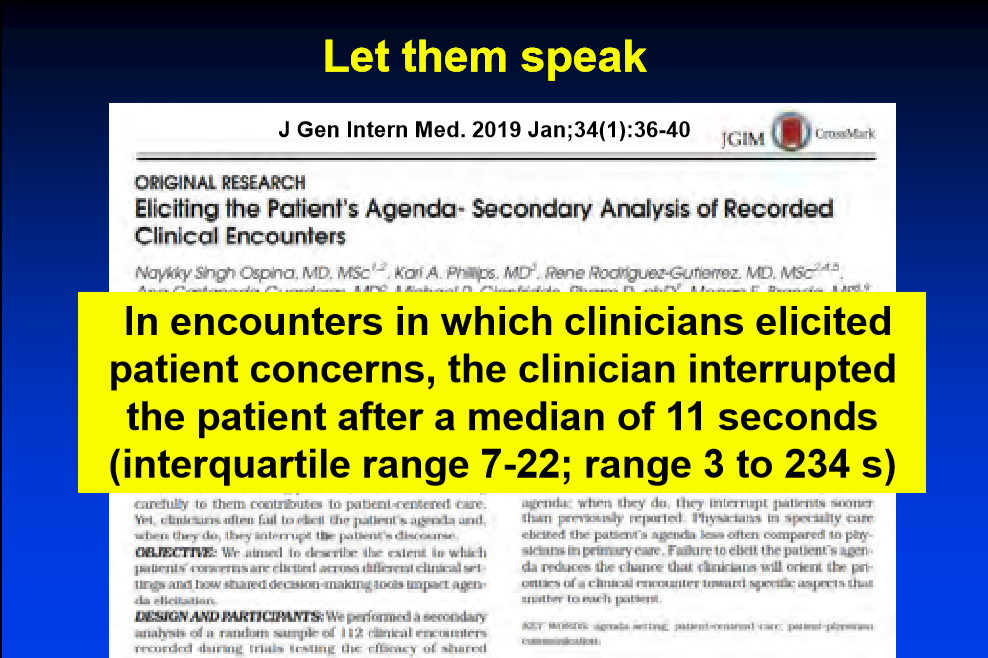
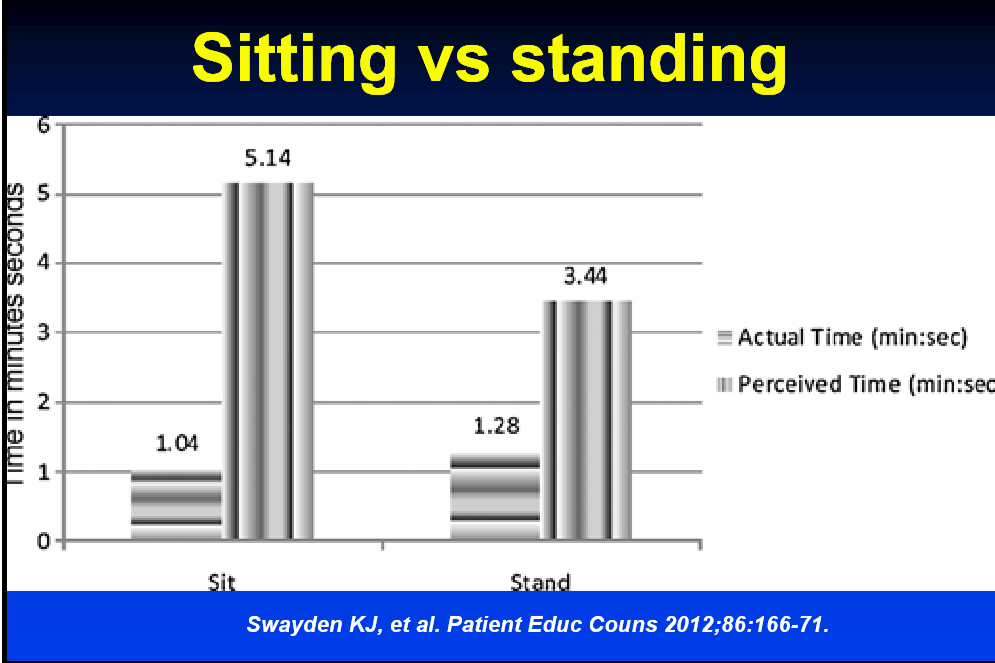
- Listen to patient and sit while listening.
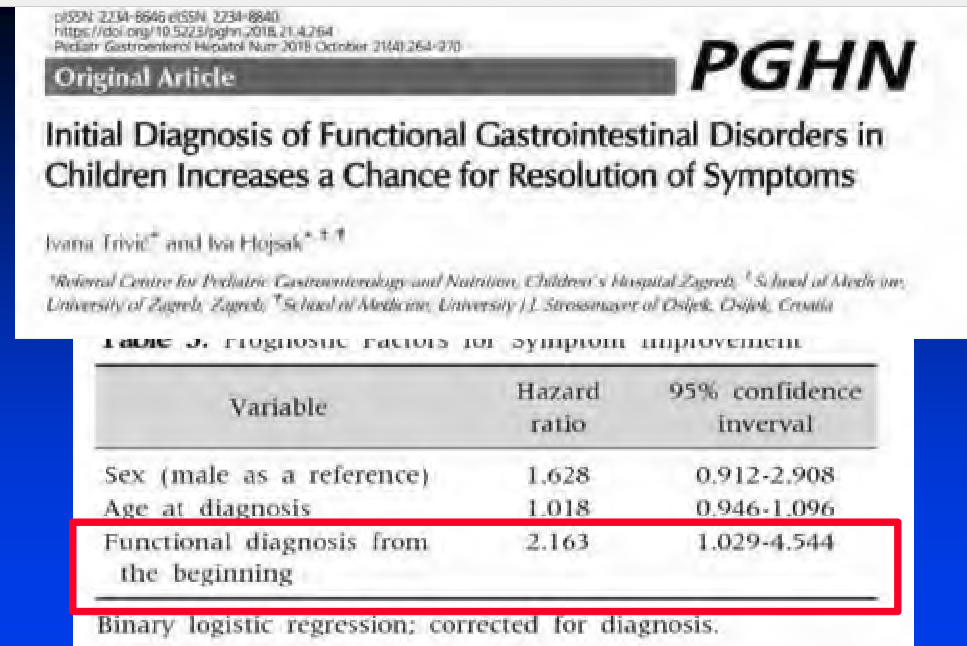
- Early diagnosis of functional disorder associated with higher long-term resolution
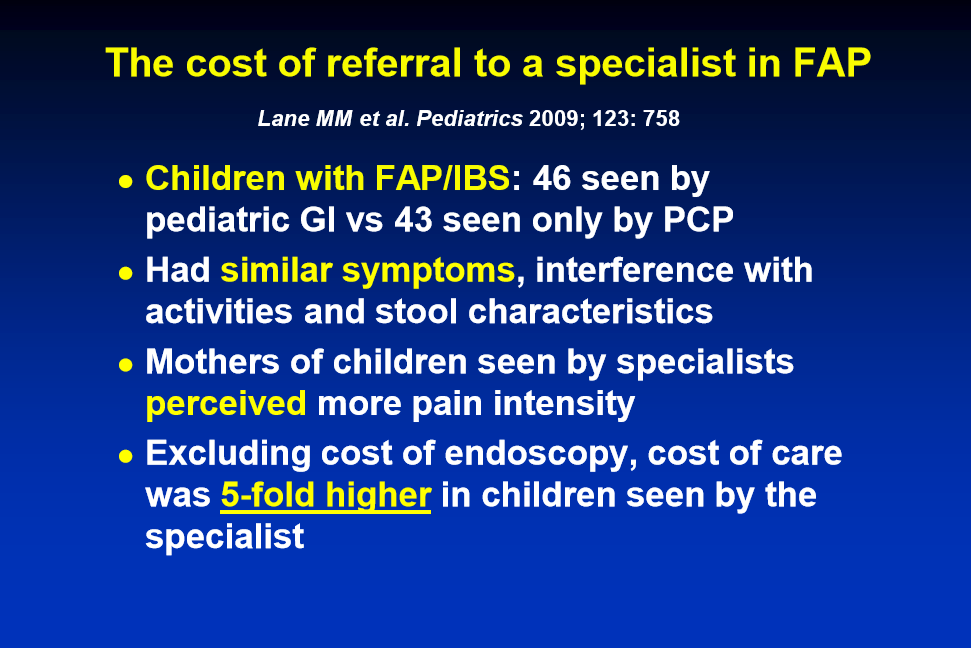
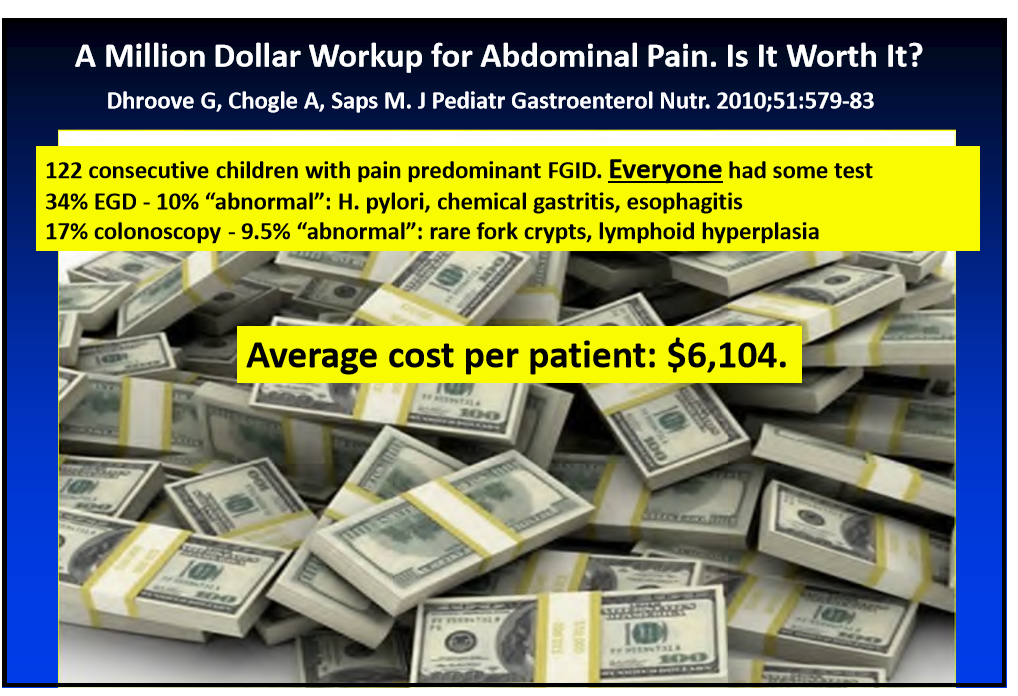
- Testing –only tests that are cost-effective: celiac disease and stool calprotectin. “Don’t get KUB for constipation.”
- Endoscopy does not improve outcomes in children with functional GI disorder (FGID)
- Eosinophilic esophagitis (EoE) treatment does not help abdominal pain but can help if patient has dysphagia
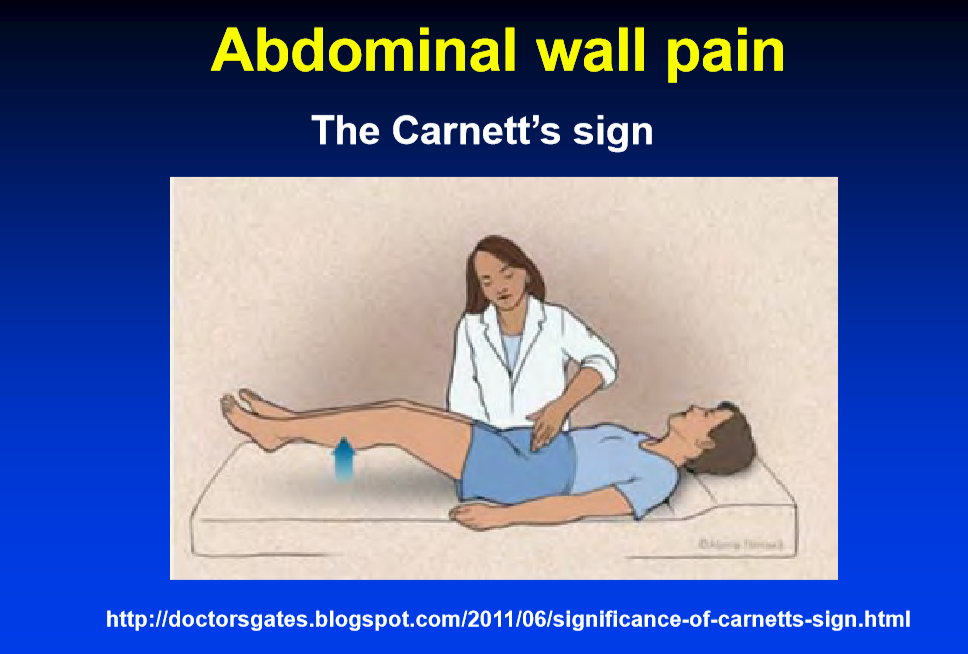
- Abdominal wall pain is often overlooked. Check Carnett sign.

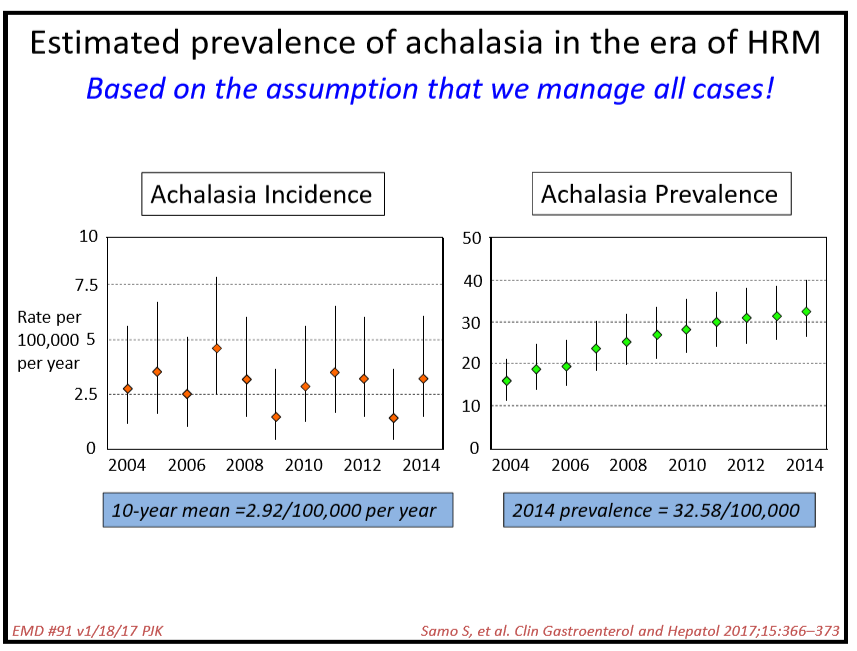
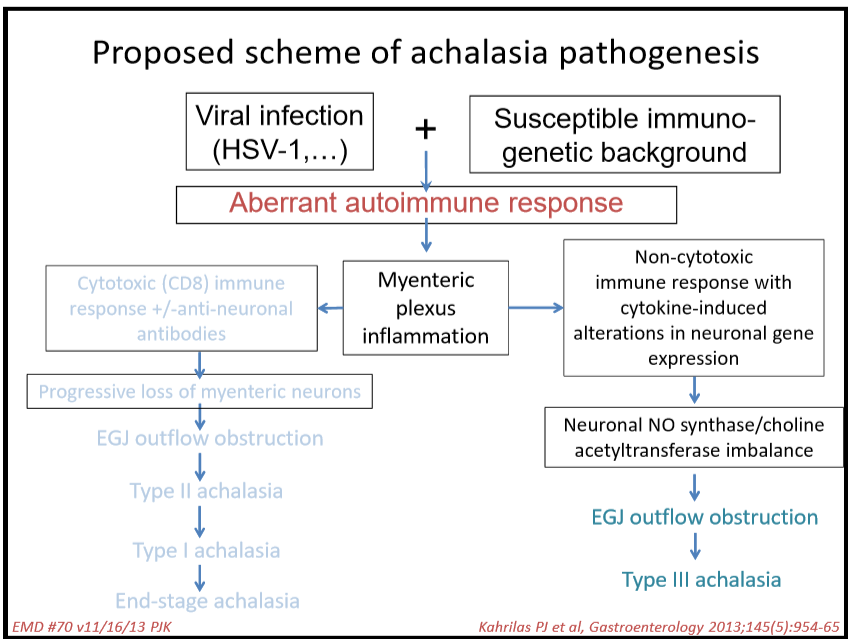
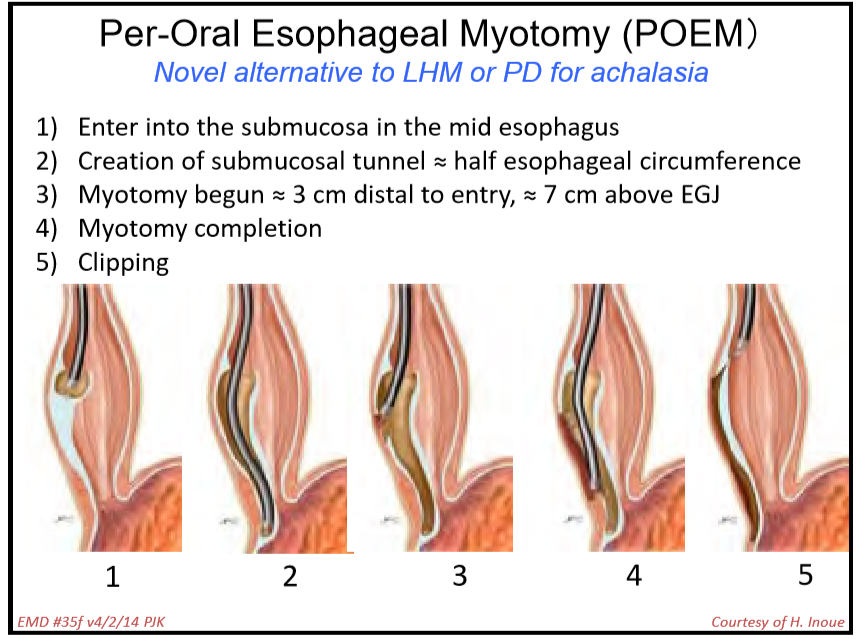
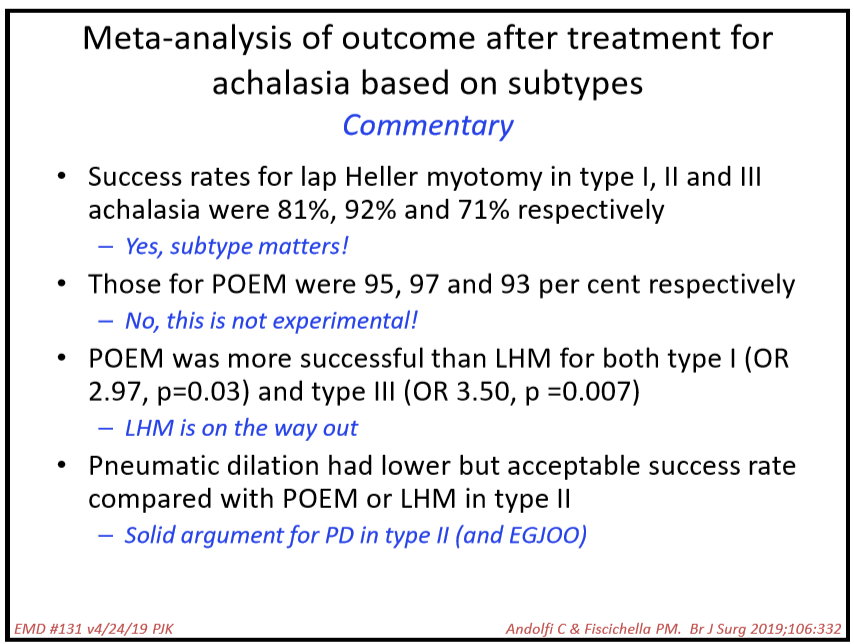
112 Peter Kahrilas, MD, Northwestern Medicine Achalasia
- Achalasia likely develops after an infection in a susceptible host
- Discussed POEM as newer treatment. It appears to be more effective than either Heller myotomy or pneumatic dilatation in adults. So far, there is limited experience in pediatrics though it appears to mirror adult experience
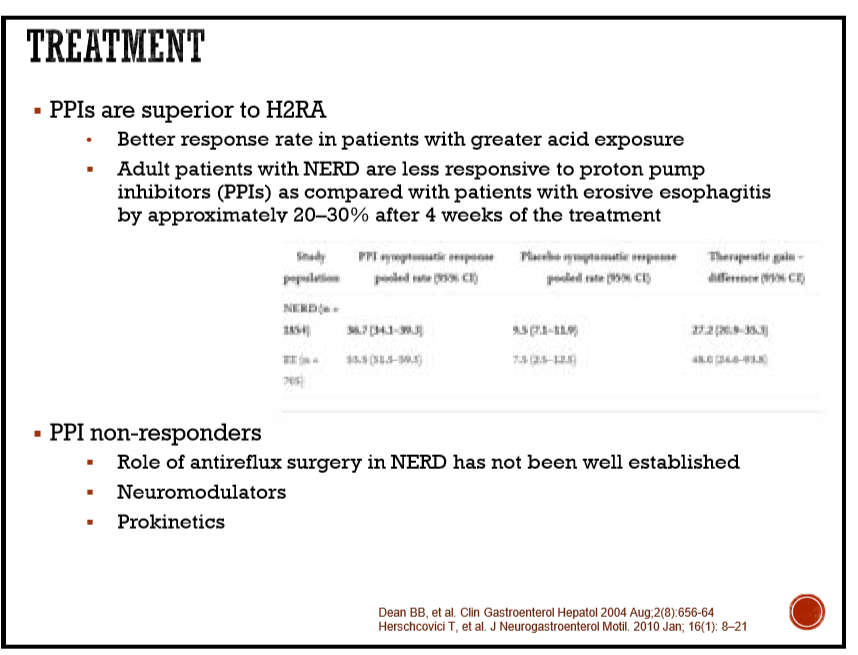
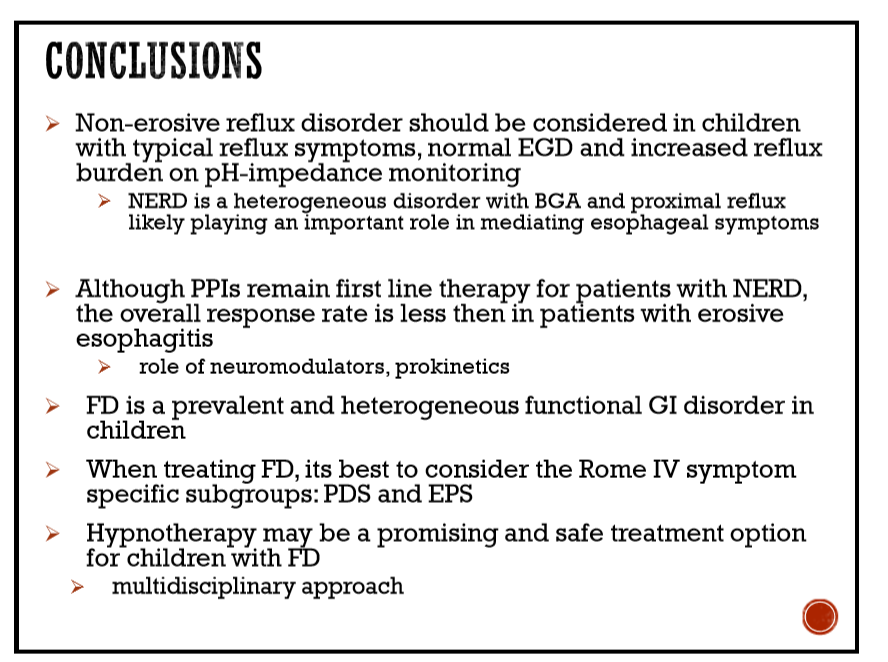
124 Julie Khlevner, MD, Morgan Stanley Children’s Hospital Evaluation and treatment strategies in NERD and functional dyspepsia
- In patients with NERD, hypermetabolizers of PPIs may need higher dosing.
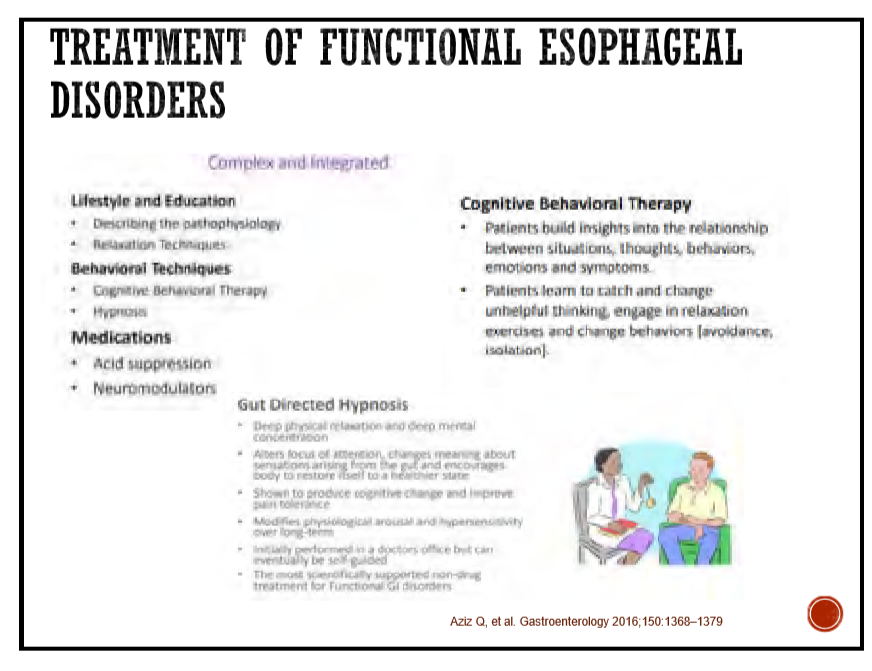
- Neuromodulators (not FDA approved) used for PPI-nonresponders. Cognitive behavioral therapies may be helpful as well.
- Functional dyspepsia with reflux symptoms are more likely to respond to PPIs than those with dyspepsia symptoms
- A Japanese herb, rikkunshito, may be helpful for functional dyspepsia
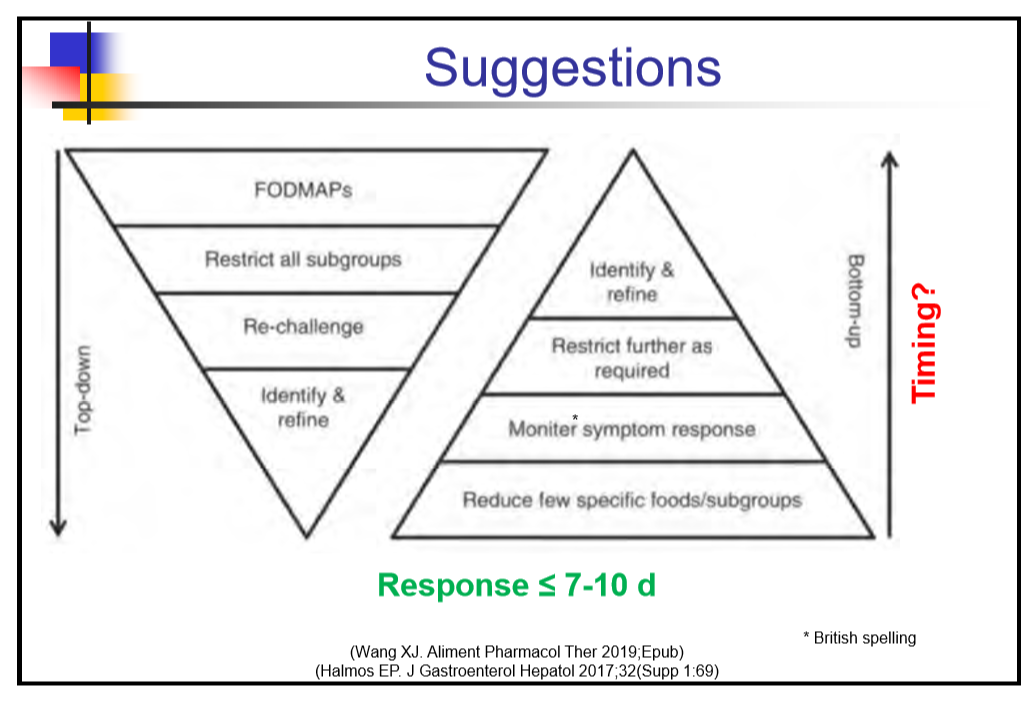
136 Robert J. Shulman, MD, Children’s Nutrition Research Center Role of diet in managing of IBS
Key points:
- Vast majority of low FODMAPs studies show “too much bias” due to lack of blinding in study designs.
- Nutritionists are needed to guide diet. Kids (families) do not follow these diets well.
- Most who are going to respond to diet will do so within 7-10 days.
Disclaimer: NASPGHAN/gutsandgrowth assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. The discussion, views, and recommendations as to medical procedures, choice of drugs and drug dosages herein are the sole responsibility of the authors. Because of rapid advances in the medical sciences, the Society cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. Some of the slides reproduced in this syllabus contain animation in the power point version. This cannot be seen in the printed version.

Pingback: Esophageal Disorders: POEM in Kids, Mitomycin C for Refractory Strictures | gutsandgrowth
Pingback: POEM vs Surgical Myotomy for Achalasia -Randomized Trial | gutsandgrowth
Pingback: Year in Review: My Favorite 2019 Posts | gutsandgrowth
Pingback: Abdominal Pain in Children Increases With Age and With Psychological Factors | gutsandgrowth
Pingback: Narrowing the Workup for Chronic Abdominal Pain –Carlo DiLorenzo Was Right! | gutsandgrowth
Pingback: Prevalence of Rome IV Functional Bowel Disorders in Adults (US, UK, Canada) & Largest Study to Date on Hydroxychloroquine for COVId-19 | gutsandgrowth
Pingback: Myth or Fact: Joint Hypermobility is Related to Pediatric Functional Abdominal Pain & Dr. Roy Link | gutsandgrowth
Pingback: “Implementing psychological therapies for gastrointestinal disorders in pediatrics” | gutsandgrowth
Pingback: Diagnostic Strategy For Children with Diarrhea and Abdominal Pain | gutsandgrowth
Pingback: Achalasia -More Complexity to Pathophysiology? | gutsandgrowth
Pingback: “Golden Half Hour in Chronic Pain” | gutsandgrowth
Pingback: Worldwide Burden of Functional Disorders | gutsandgrowth
Pingback: Prospective Pediatric Study of the Persistence and Progression of Recurrent Abdominal Pain | gutsandgrowth
Pingback: Carlo DiLorenzo: Lessons Learnt Over 30 Years | gutsandgrowth
Pingback: Course of Functional Abdominal Pain Before and During Pandemic | gutsandgrowth