
SK Murthy et al. Gastroenterol 2021: DOI:https://doi.org/10.1053/j.gastro.2021.05.063. Full Text: AGA Clinical Practice Update on Endoscopic Surveillance and Management of Colorectal Dysplasia in Inflammatory Bowel Diseases: Expert Review

Some of the recommendations:
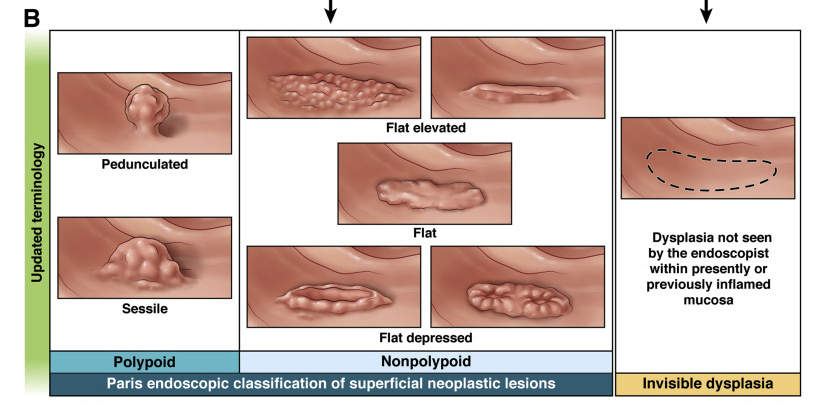
Best Practice Advice 1: Precancerous colorectal lesions in inflammatory bowel disease should be described as either polypoid (≥2.5 mm tall), nonpolypoid (<2.5 mm), or invisible (detected on nontargeted biopsy), using a modified Paris Classification. The older terms dysplasia-associated lesion or mass, adenoma-like mass, and flat dysplasia (when referring to dysplasia detected in nontargeted biopsies) should be abandoned.
Best Practice Advice 3: Initial colonoscopy screening for dysplasia should be performed at 8–10 years after disease diagnosis in all people with colonic inflammatory bowel disease, and immediately on diagnosis of primary sclerosing cholangitis. Staging biopsies should be taken from multiple colonic segments to assess histologic disease activity and extent and to help guide future surveillance intervals.
Best Practice Advice 8: Extensive nontargeted biopsies (roughly 4 adequately spaced biopsies every 10 cm) should be taken from flat colorectal mucosa in areas previously affected by colitis when white light endoscopy is used without dye spray chromoendoscopy or virtual chromoendoscopy. Additional biopsies should be taken from areas of prior dysplasia or poor mucosal visibility. Nontargeted biopsies are not routinely required if dye spray chromoendoscopy or virtual chromoendoscopy is performed using a high-defintion endoscope, but should be considered if there is a history of dysplasia or primary sclerosing cholangitis.

