KH Allin, P Moayyedi. Gastroenterol 2021; 161: 1789-191 (editorial). Open Access: Proton Pump Inhibitor Use: A Risk Factor for Inflammatory Bowel Disease or an Innocent Bystander?
This editorial helps provide needed context on the associated observational study by Xia et al (B Xia, M Yang et al. Gastroenterol 2021; 161: 1842-1852. Open Access. Regular use of proton pump inhibitor and the risk of inflammatory bowel disease: pooled analysis of 3 prospective cohorts) which showed a mild increase risk of IBD among PPI users. While the PPI users were at 42% increased risk of IBD compared to nonusers, if correct, “the absolute risk associated with PPI use is modest. Number needed to harm is 3770, meaning that when 3770 individuals are treated with PPIs for 1 year, 1 additional case of IBD is observed.”
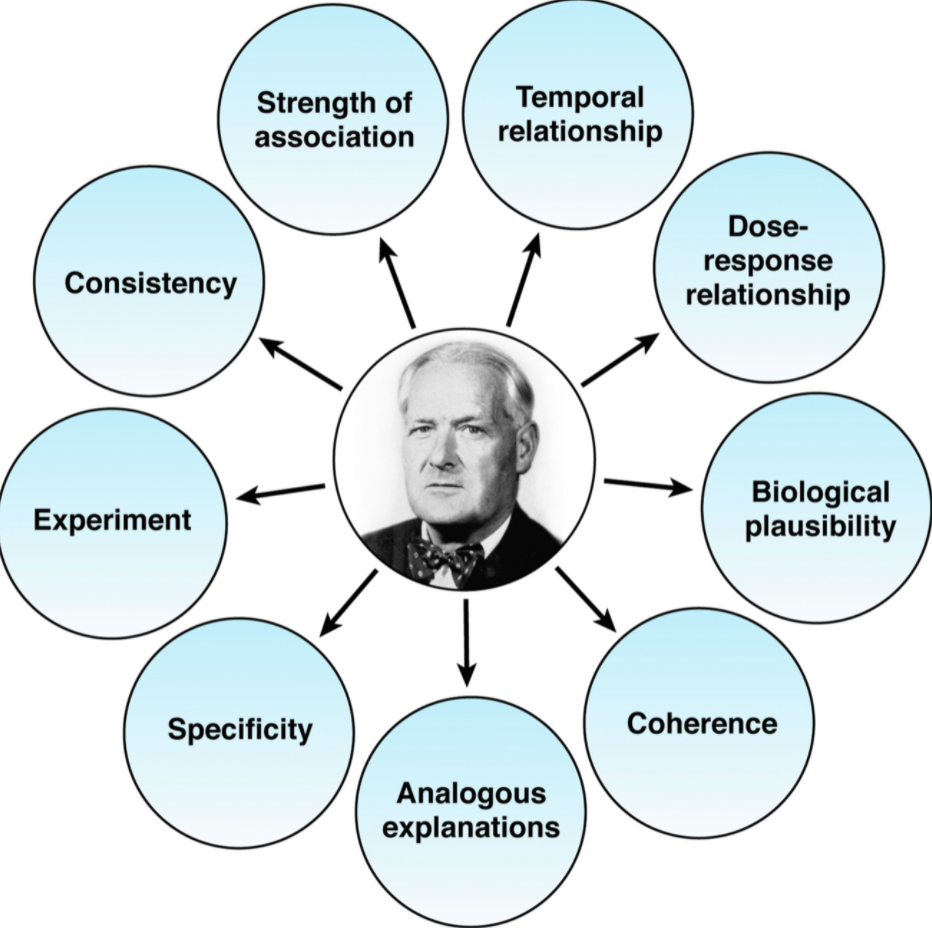
Despite the efforts of the study authors to minimize confounders, the editorial focuses on the work of Austin Bradford Hill (Proc R Soc Med. 1965; 58: 295-300. The environment and disease: association or causation?) who “realized making causal inferences on observational data was challenging and outlined a list of factors that would make this interpretation more or less likely….strength of association, dose response, and consistency are important and often not commented on in observational studies.”
In a previous “a double-blind, randomized clinical trial comparing pantoprazole with placebo over 3 years with more than 53,000 patient years follow-up found there was no association” with IBD identified…Interestingly, this trial reported a slightly higher risk of enteric infections, and this is the underlying mechanism proposed for how PPI therapy may increase the risk of IBD.”
My take (borrowed from editorial): “Most associations for PPI and harm are likely to be residual or unmeasured confounding, whether this is also true for IBD will only be determined by further study.”
Related blog posts:
- Why Observational Studies Are Misleading & PPI Association with Kidney Stones
- PPIs: Good News on Safety
- PPIs: Good News on Safety (Part 2) | gutsandgrowth
- More Good News for PPIs: NO Increased Risk of Dementia
- Deconstructing PPI-Associated Risks with Nearly 8 Billion Data Points and More on COVID-19 GI Symptoms (Video) | gutsandgrowth
- PPI Side Effects: “Dissecting the Evidence” | gutsandgrowth