
JE Squires et al. JPGN 2022 – Volume 74 – Issue 1 – p 138-158. doi: 10.1097/MPG.0000000000003268. Open Access: North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition Position Paper on the Diagnosis and Management of Pediatric Acute Liver Failure
This article provides a terrific summary of the most urgent issues with regard to caring for children with PALF; this article provides helpful information for diagnosis, and management, as well as information on pathophysiology, and associated outcomes.
PDF version: PALF in Children Position Paper
The article makes a number of recommendations for testing/treatment -here are a few of them:
- While the initial testing does list ferritin, it does not list soluble IL2R as an early test (listed lower in Table 4 under section of hepatic encephalopathy). My colleagues at Emory who specialize in liver transplantation have frequently recommended this test early in the evaluation of severe liver disease/acute liver failure (ALF) as a potential marker of HLH and immune dysregulation.
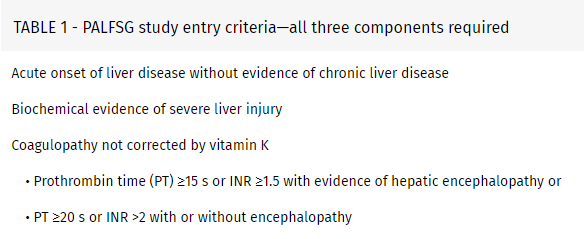
- With regard to coagulopathy: “Coagulopathy secondary to vitamin K deficiency should rapidly correct following appropriate repletion. Notably, if coagulopathy persists, efforts to “correct” abnormal coagulation profiles with fresh frozen plasma or other pro-coagulation products should generally be avoided” [in the absence of bleeding or need for invasive procedure].
- Initial IV Fluids: ” In the absence of the need for volume resuscitation, total intravenous fluids should initially be restricted to around 90% of maintenance fluids to avoid overhydration. Initial fluids should be similar to hypertonic glucose (D10) one-half normal saline and supplemented with 15 mEq of potassium (K+)/L.”
- Nutritional support: “Patients with PALF are likely catabolic and require more calories than basal needs. Enteral feeding is often preferred over total parenteral nutrition (TPN), and both naso-gastric or naso-jejunal feeds should be considered before TPN.”
- Neonatal ALF: “GALD results from an intrauterine alloimmune liver injury and is suspected to be the single most common cause of neonatal acute liver failure… Characteristic clinical features of GALD include an ALF presentation usually at birth and almost always in the first days of life. The majority (70–90%) of affected infants are born premature and a history of maternal sibling death is common. Timely exchange transfusion and high-dose intravenous immunoglobulin (IVIG) is the preferred treatment to remove offending antibodies and block their action, including activation of complement (88,91). The mechanism of GALD places subsequent pregnancies at risk, and intrapartum IVIG should be used to prevent recurrences.”
- Table 8 list common medications implicated in PALF. “Acetaminophen (APAP) …remains the most common cause of DILI, and is the most common identified cause of ALF in children.”
Related blog posts:
- Acute Liver Failure -Pediatric ICU Management
- Time to Adjust the Knowledge Doubling Curve in Hepatology In this post, AASLD expert guidance: for platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count.” For INR in setting of cirrhosis: “The INR should not be used to gauge procedural bleeding risk in patients with cirrhosis who are not taking vitamin K antagonists (VKAs)…Measures aimed at reducing the INR are not recommended before procedures in patients with cirrhosis who are not taking VKAs…FFP transfusion before procedures is associated with risks and no proven benefits.”
- Genetic Underpinnings of Acute Liver Failure in Children
- Recurrent Acute Liver Failure Due to NBAS Deficiency
- Algorithm for Neonatal Acute Liver Failure
- Changing Approach to Neonatal Acute Liver Failure
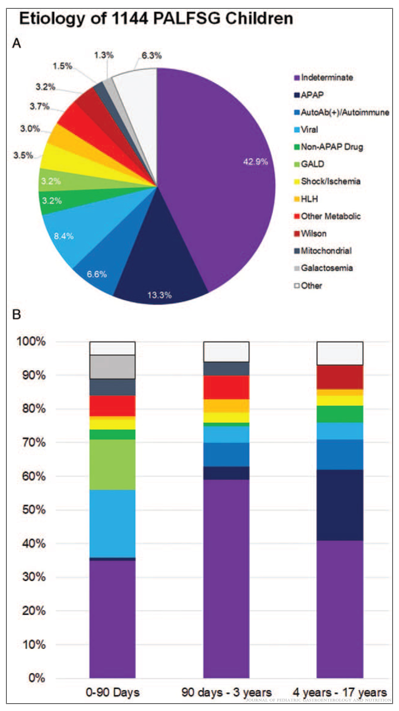
(A) Etiology for 1144 children from the Pediatric Acute Liver Failure Study Group (PALFSG) 1999–2014. (B) Final diagnosis by age (note: figure B includes information on only 985 participants)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
