
Yesterday’s link to a funny 2 minute eulogy did not work right and has been fixed. Here is the updated link and it should work: Humor: Eulogy
In response to this video, Steven Liu sent me a link to a a Weird Al Yankovic:YouTube: Word Crimes. This link would probably be helpful for those reviewing a poorly-written journal submission when providing feedback (& hopefully not sent to anyone trying to provide information via a GI blog).
————-
USA Today (8/9/22): Fewer than a third of insured Americans with hepatitis C receive timely treatment, CDC study shows
“More than 95% of people infected with hepatitis C can be cured with a simple course of antivirals…[the CDC] looked at nearly 50,000 insured patients diagnosed with hepatitis C between January 2019 and October 2020 and found less than one-third received treatment within a year of their diagnosis, according to the study published Tuesday in the Morbidity and Mortality Weekly Report...Treatment was lowest among patients who had state-administered Medicaid plans, with about 23% receiving it. About 28% people covered by Medicare and 35% with private insurance received treatment within the year.”
“Cases of hepatitis C rates have skyrocketed as the opioid epidemic worsens, jumping from an estimated 2,700 infections in 2011 to 57,500 infections in 2019, according to the CDC.”
NY Times (7/26/22): Viral Infections and Gene Variant Are Linked to Child Hepatitis Cases
“Two small studies…suggest a possible explanation for the hepatitis cases: In a small subset of children with this particular gene variant, dual infections with A.A.V.2. (adeno-associated virus 2) and a helper virus, often an adenovirus, trigger an abnormal immune response that damages the liver….As of July 8, 1,010 probable cases had been reported from 35 countries, according to the World Health Organization”
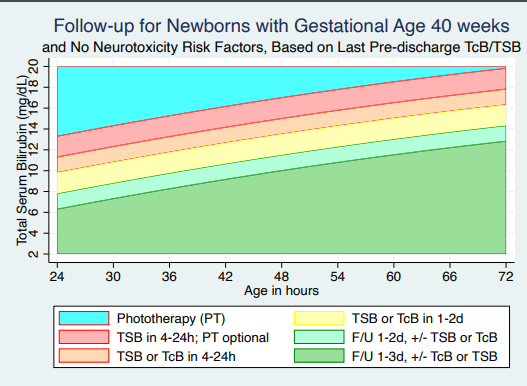
AR Kemper et al. Pediatrics 2022; https://doi.org/10.1542/peds.2022-058859. Open Access: Clinical Practice Guideline Revision: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation
- Graphs showing follow-up recommendations by gestational age and presence of neurotoxicity risk factors
- One of these graphs below:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
