
Thanks to Ben Gold for this reference.
AC Ford et al. The Lancet 2023; DOI:https://doi.org/10.1016/S0140-6736(23)01523-4. Open Access! Amitriptyline at Low-Dose and Titrated for Irritable Bowel Syndrome as Second-Line Treatment in primary care (ATLANTIS): a randomised, double-blind, placebo-controlled, phase 3 trial
In this randomized, double-blind, placebo-controlled study of 463 adults (median age 48 yrs), the authors compared low-dose oral amitriptyline (10 mg once daily) or placebo for 6 months, with dose titration over 3 weeks (up to 30 mg once daily). The use of the Rome IV criteria resulted in the selection of a group of patients with higher symptom severity,50 borne out by the mean IBS-SSS scores at baseline, which were in the moderate to severe range. The median duration of IBS among participants was 10 years.
Key findings:
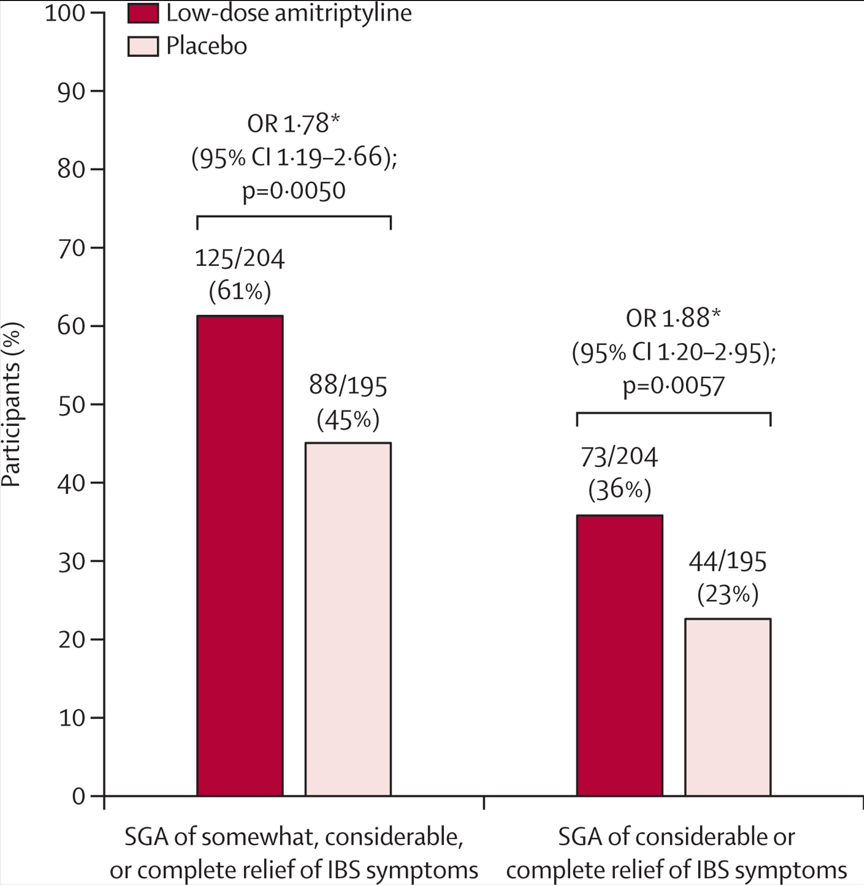
- Intention-to-treat analysis of the primary outcome showed a significant difference in favour of low-dose amitriptyline in IBS-SSS score between groups at 6 months (–27·0, 95% CI –46·9 to –7·10; p=0·0079)
- 46 (20%) participants discontinued low-dose amitriptyline (30 [13%] due to adverse events), and 59 (26%) discontinued placebo (20 [9%] due to adverse events) before 6 months.
In their discussion, the authors note that “this is the largest trial of a tricyclic antidepressant in IBS ever undertaken and the first based entirely in a primary care setting…low-dose amitriptyline met the primary outcome, with a mean decrease in IBS-SSS of almost 100 points at both months 3 and 6 compared with baseline, and also met the key secondary outcome for effectiveness, as well as other IBS symptom measures.”
“There was no effect of low-dose amitriptyline on somatoform symptom-reporting scores, or anxiety or depression scores, during 6 month follow-up, nor was there any impact on work and social activities.:
My take (borrowed from authors): Titrated low-dose amitriptyline was superior to placebo as a second-line treatment for IBS in primary care across multiple outcomes, and was safe and well tolerated.
Related blog posts:
- “How to Approach a Patient with Difficult-to-Treat IBS” (2021)
- Topamax and Amitriptyline Did Not Work for Pediatric Migraines
- A 6-Year Study of Amitriptyline, Escitalopram, and Functional Dyspepsia
- Patient Information on Irritable Bowel (Rome Foundation)
- Advice on Abdominal Pain for Everyone Who Cares for Children | gutsandgrowth
- Brave New World: Psychotropic Medications and Pediatric Functional GI Disorders
- NY Times: “Millions Take Gabapentin for Pain. But There’s Scant Evidence It Works.” | gutsandgrowth
- Gut-Brain Modulators for Functional GI Disorders: Irritable Bowel, Dyspepsia, Functional Heartburn, and Cyclic Vomiting Syndrome
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
