
Dr. Goday gave our group a great lecture on pediatric feeding disorders. I’ve included many of his slides along with some of my notes. There may be errors in omission and transcription on my part.
Feeding tubes:
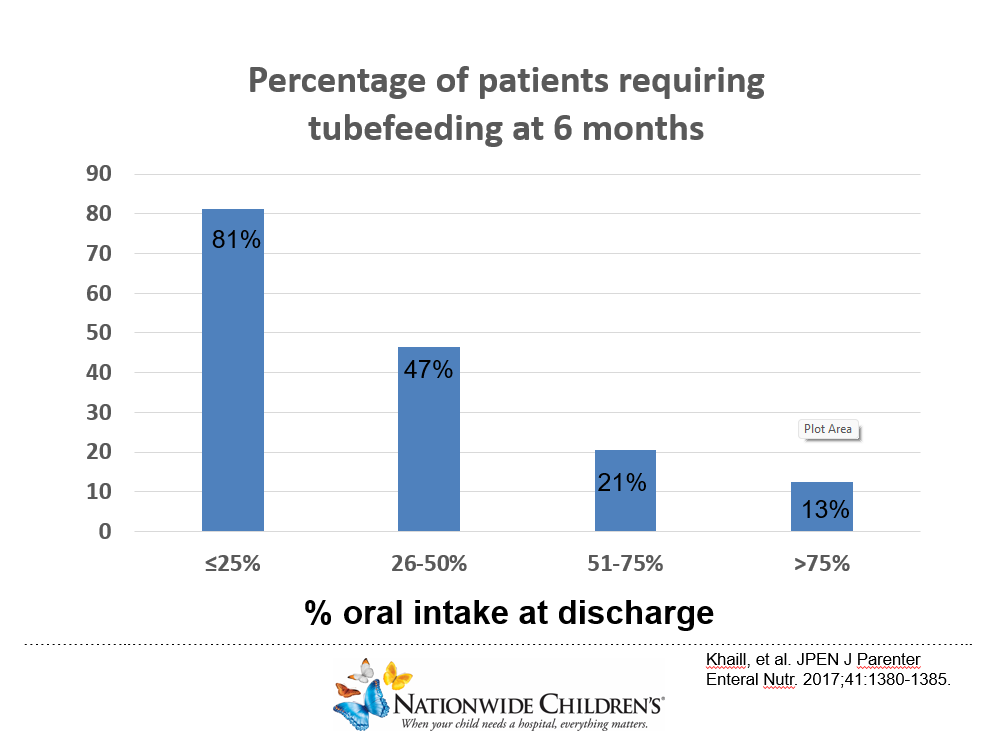
- If taking >75% of feeds orally, only 13% still needing tube feeds 6 months later. If taking <25%, 81% still needing tube feeds 6 months later (needs a GT)
- Bridle: Dr. Goday recommends using up to 8 weeks. If needing longer, GT placement is recommended
- If needing an NG tube more than 3 months (possibly 6 months), GT placement is recommended
- Pre-op studies are not predictive of who will need GJ feedings vs GT feedings




Medications:
- Cyproheptadine -Dr. Goday prefers single night time dose, usually cycles medicine (2 weeks on, 1 week off), uses as early as 8 months of age. Watch for adverse effects on behavior.
- Mirtazapine -often used in older children and adolescents though effects on appetite wane with usage. Dosed as an oral disintegrating tablet. Typically, 7.5 mg in older children and 15 mg in adolescents.
- Vitamins -Gummy vitamins are NOT complete vitamins, Nano VM -minimal taste powder (costly)

Choking phobia
- Can occur with pharyngitis
- Usually needs EGD and sometimes anxiolytic

Formulas:
- No clear nutritional role for toddler step-up formulas
- Dr. Goday often will use infant formula between 1-2 yrs of life rather than pediasure in those without growth concerns. Pediasure may reduce acceptance of solid foods (due to its sweet taste)
- Get help from your nutritionists in kids with limited diets
Autism:
- Avoid adding medication/vitamins to the ‘one food/formula that child will take.’ He may stop taking that food/formula too
Related blog posts:
- Food Selectivity in Children with Autism
- Mel Heyman: Past, Present and Future of ARFID
- Highly Prevalent Pediatric Feeding Disorders
- Data on Bridles -They Work!
- Fundamentals of Gastrostomy Tubes
- Impact of NG Feeding Program for NICU Graduates
- N2U -Part 2: Poor Growth and Short Bowel Syndrome
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
