
R Paknikar et al. NEJM 2023; 389: 1321-1326. Digging into the Histology
In this case report, a 33-year-old man (from the midwest) with ulcerative colitis (diagnosis seven years prior) who was receiving treatment with tofacitinib (a Janus kinase inhibitor) presented to the hospital with fatigue (x 8 months) and bloody diarrhea. He also had had fevers (x 4 months), 23 lb weight loss, and drenching night sweats. Before tofacitinib, treatment had included adalimumab and azathioprine. He had undergone a sigmoidoscopy two months prior to presentation.
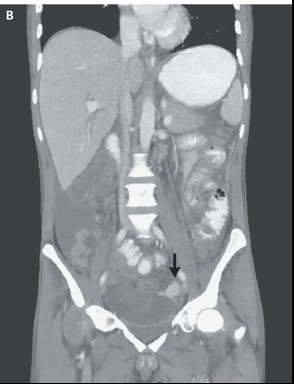
His workup included a CXR showing diffuse reticulonodular opacities, a CT scan showing thickening in the colon and extensive infection workup. On the third hospital day, he had a perforation and resection which led to the diagnosis of invasive histoplasmosis.
My take: This article is useful for understanding how to workup secondary infections in IBD patients on long-term immunosuppressive agents.
One example: “testing for 1,3-β-d-glucan can serve as an adjunctive test for invasive fungal infections caused by fungi expressing 1,3-β-d-glucan in their cell walls, including candida, aspergillus, Pneumocystis jirovecii, Histoplasma capsulatum, and coccidioides; such testing has a high negative predictive value for infection with these organisms. In contrast, cryptococcus and blastomyces produce very low levels of 1,3-β-d-glucan in their cell walls and are therefore not readily detected by serum testing for the cell-wall antigen.”
Related blog posts:
