Briefly noted: S Sanagapalli et al. The American Journal of Gastroenterology 120(9):p 2051-2058, September 2025. Prospective Controlled Study of Endoscopic Botulinum Toxin Injection for Retrograde Cricopharyngeus Dysfunction: The Inability to Belch Syndrome
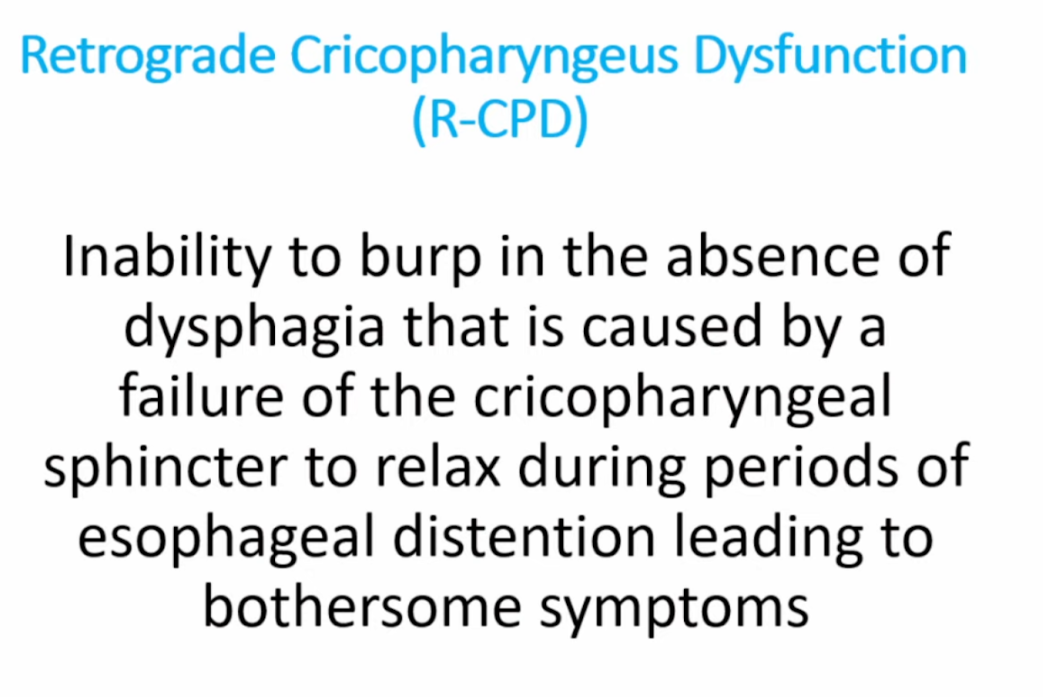
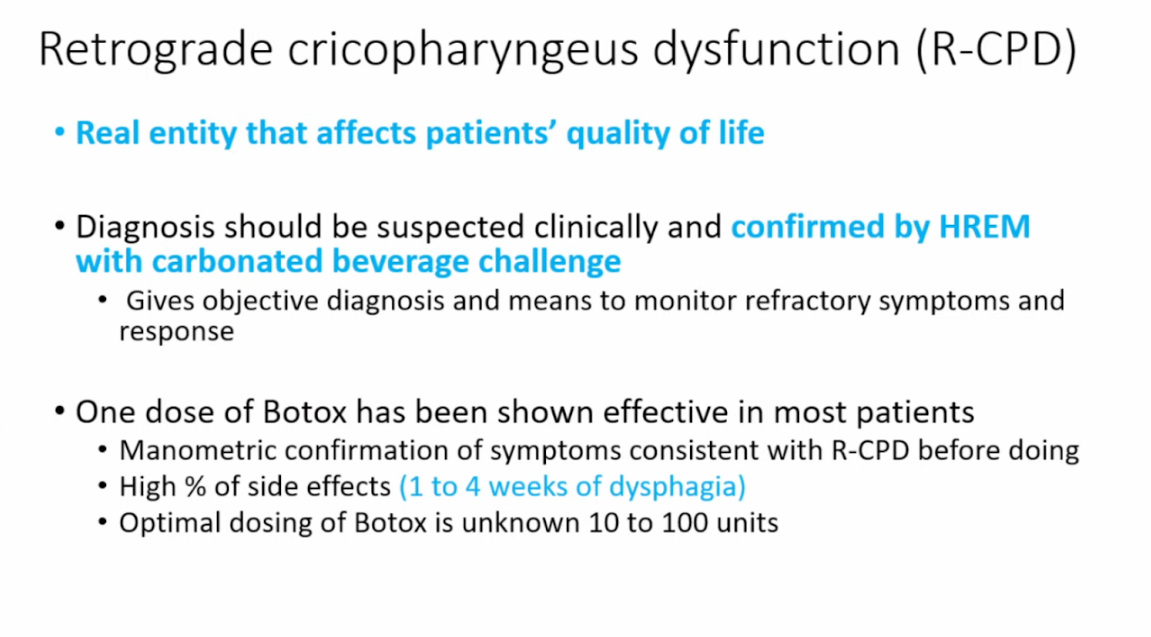
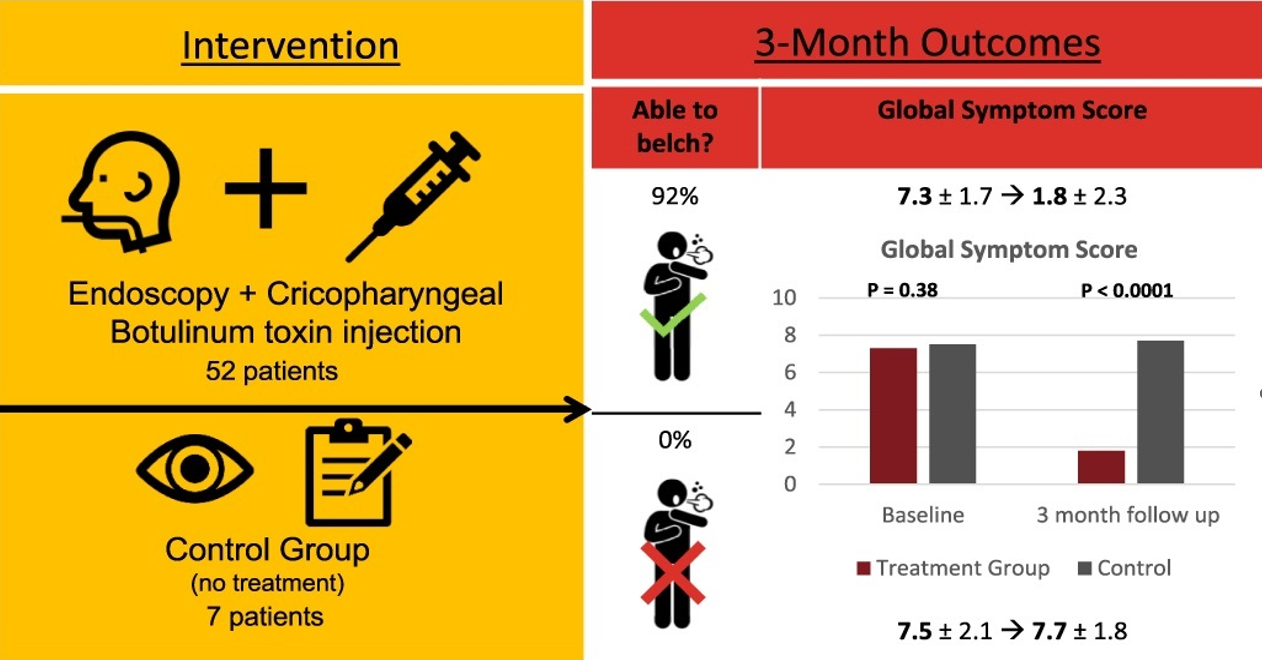
This study explored a treatment with botulinum toxin (aka. Botox) for people who can’t belch due to a condition called retrograde cricopharyngeus dysfunction (R-CPD), which causes gas-related discomfort. Researchers used high-resolution manometry (HRM) with carbonated drink provocation to diagnose R-CPD. Then, they tested a treatment involving botulinum toxin injections into the cricopharyngeal muscle.
Out of 65 participants, 52 received the treatment, and 92% of those who received the treatment were able to belch after three months, significantly improving their symptoms and quality of life. In contrast, the control group, which included participants who deferred or declined treatment, saw no improvement. After 3 months, 43/51 (84%) of the treatment group reported being satisfied or very satisfied with therapeutic outcome.
Related blog posts: