
H Khalili et al. Annals of Internal Medicine 2025; https://doi.org/10.7326/ANNALS-25-0026. Medications and Risk for Microscopic Colitis: A Nationwide Study of Older Adults in Sweden
Methods: The authors used Total Population Register, which includes information on the age and sex of all residents in Sweden. Then the cohort of older adults in Sweden was linked to the ESPRESSO study), which contains data on GI-related biopsies from all 28 pathology departments in Sweden from January 1965 until April 2017.
Key findings:
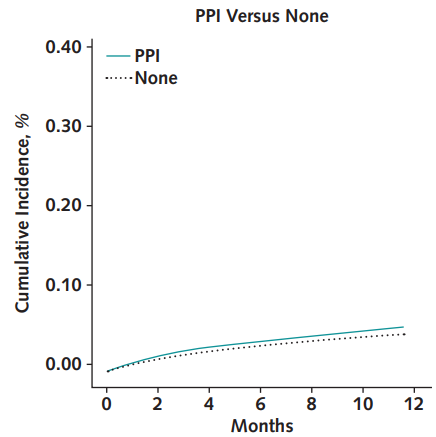
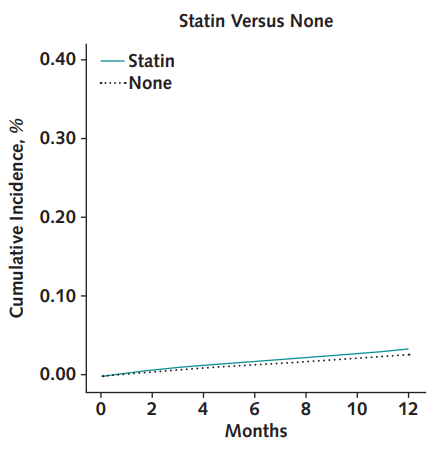
- Estimated 12-month risk differences were close to null under angiotensin-converting enzyme versus calcium-channel blocker (CCB) initiation, angiotensin-receptor blocker versus CCB initiation, nonsteroidal anti-inflammatory drug initiation versus noninitiation, proton-pump inhibitor initiation versus noninitiation, and statin initiation versus noninitiation.
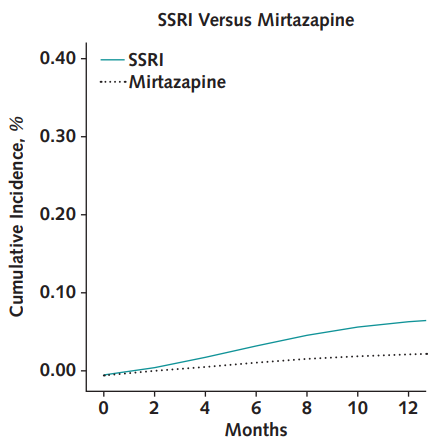
- There was a slight increase risk of microscopic colitis in patients receiving SSRIs compared to mirtazapine. The estimated 12-month risk difference was 0.04% (95% CI, 0.03% to 0.05%) for selective serotonin receptor inhibitors (SSRIs) versus mirtazapine.
- Several medications were also associated with increased risk for receiving a colonoscopy with a normal colorectal mucosa biopsy result.

My take: Microscopic colitis is a very infrequent problem in the pediatric population. With the exception of SSRIs, this study in older adults did not find a significant relationship between purported “trigger” medications and the development of microscopic colitis. In addition, the low persistent associations with SSRI initiation may be due to surveillance bias.


