
AL Miller et al. Dysphagia 2024; 39: 33-42. Predictive Value of Laryngeal Penetration to Aspiration in a Cohort of Pediatric Patients
This was a retrospective study with 97 patients over a 6 month period in 2018. The authors note that “there is no universally accepted protocol for pediatric video swallows across ages and conditions.”
Methods: Depth of penetration and/or aspiration and reaction were classified according to the 8-point Penetration–Aspiration scale [JC Rosenbek, et al. Dysphagia 11, 93–98 (1996). https://doi.org/10.1007/BF00417897]. The frequency of penetration events and aspiration was grouped into categories: none (1); infrequent or occasional episodes (at least 1 event to less than 30%) (2); intermittent episodes (30–40% of total swallows) (3); frequent episodes
(50% or greater of total swallows) (4). Data for all swallowing parameters was stratified by bolus type (thin liquid, thickened liquid, puree solid). All VFSS were independently
scored by two speech-language pathologists and two radiologists.
Key findings:
- Aspiration was seen in 21% of patients (n=20 of 97).
- Penetration events were more frequent and occurred in 64% of participants (n=62 of 97). . Of patients with any penetration events, 30% also had documented aspiration
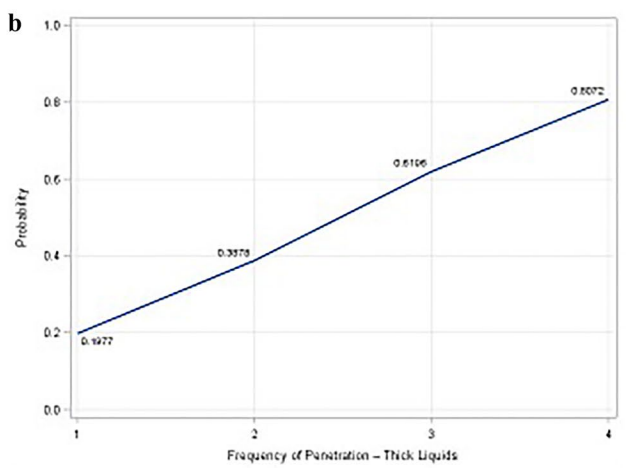
- Frequency of penetration and aspiration: 80% of patients showing frequent penetration [frequency 4] demonstrating aspiration compared to 2.3% of patients with isolated penetration [frequency 1]. There was a higher risk of aspiration at lower frequency penetration if this occurred with thicker liquids (see below)
- Depth of penetration and aspiration:. For patients with penetration contacting the vocal folds [depth 5], nearly 95% demonstrated documented aspiration within the same study; however, those with depths 1-3 had minimal risk of aspiration (see below). There was a higher risk of aspiration at shallow depths with thicker liquids.




My take (borrowed from authors): “children with shallow, intermittent penetration events
without associated aspiration are likely to be demonstrating clinically insignificant events. Such children are therefore not appropriate candidates for compensatory or alternative feeding strategies such as changes in mode of delivery (e.g., gastrostomy tube), alteration of flow rate, or modification of liquid viscosity, such as thickened feedings.”
Related blog posts:
- Can We Ignore Laryngeal Penetration?
- Clinical Evaluation Not Sensitive for Aspiration
- Something Useful for Apparent Life-Threatening Events (ALTEs) [or BRUEs]
- What to do with ALTEs
- Does Reflux Lead to Increased Aspiration Pneumonia?
- NASPGHAN Dysphagia Webinar: Dr. Khalil El-Chammas, Dr. Peter Osgood, and Dr. Jose Garza

