
“The best preparation for tomorrow is to do today’s work superbly well” –William Osler (quote cited in NEJM 2014; 371: 1565-66).
This blog entry has abbreviated/summarized the presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
For me, these lectures were a useful review and represent an effort to achieve Osler’s objective of doing superb work. If I had to choose a single issue that may affect my practice: when initiating infliximab, consider checking week 14 trough levels of infliximab and optimize dosing.
The role of the microbiome in IBD –Subra Kugathasan (Emory)
This was a terrific lecture though with some overlap with a number of other presentations at the meeting. The lecture reviewed how to interpret microbiome studies and what we are learning from these studies with regard to inflammatory bowel disease.
Enteral Nutrition and Microbiota –conclusion:
- EN may work by suppressing the entire microbiota in Crohn’s disease thus lowering antigenic effect to the gut
- Some microbes may be pro-inflammatory and others pro-fibrotic
- Chicken and egg: preliminary evidence suggests that dysbiosis is probably a preceding predisposing factor rather than due to the consequence of having inflammatory bowel disease.
The Role of Drug Monitoring in Inflammatory Bowel Disease –Jennifer Strople (Children’s Hospital of Chicago)
TPMT Testing/thiopurine metabolite monitoring
- goal: minimize adverse effects and optimize thiopurine dosing.
- those with lower (but not absent) activity may be best candidates for treatment with azathioprine/6-mercaptopurine (thiopurines).
- normal TPMT testing does NOT exclude complications like bone marrow suppression or pancreatitis.
- obtaining TPMT at baseline is cost-effective
- goal of 6-thioguanine level of >235 (odds ratio favorable of responding to/remission with treatment)
- drug levels: allows monitoring for noncompliance; limitation of costs and using levels inappropriately. Routine testing “has no role in patients who are doing well on acceptable doses of thiopurines”
- younger patients often need higher doses
Monitoring for anti-TNF Therapy
- Loss of response most common in first year of therapy.
- For infliximab (IFX), IFX trough levels >3 mcg/mL predicted sustained response. Gut 2014; 63: 1721.
- Week 14 IFX levels predict outcomes:
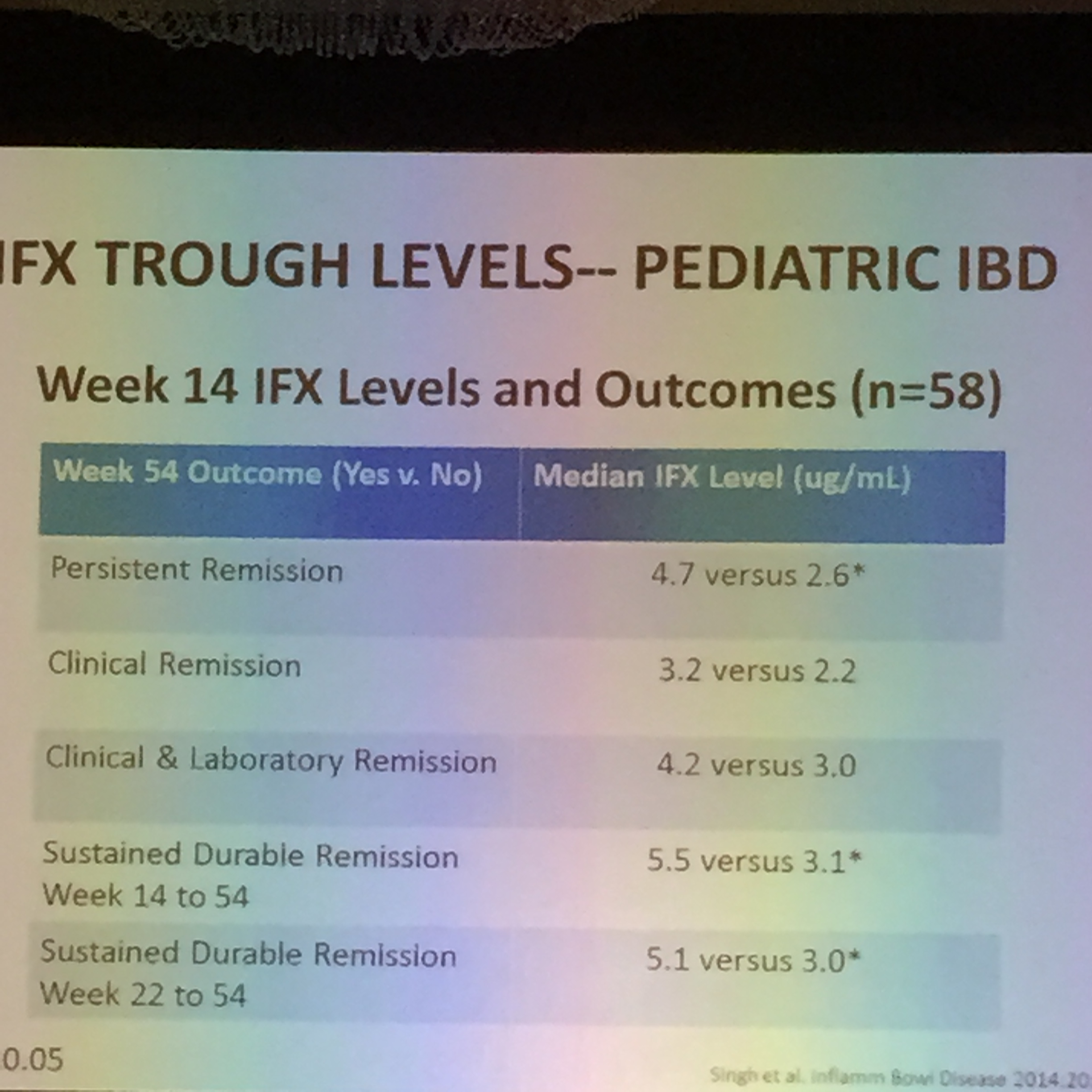
IFX Levels at 14 weeks
- Preliminary data with ulcerative colitis shows that troughs >3.7 mcg/mL increases likelihood of mucosal healing and remission.
- Undetectable trough levels of IFX associated with increased risk of colectomy with ulcerative colitis Gut 2010 59: 49
- If a patient develops high levels of anti-drug antibodies (ADAs), this makes likelihood of response to medications unlikely. The specific ADA level is helpful; high levels of drug antibody are particularly problematic. If low levels of drug without ADAs, then increasing dose is typically effective.
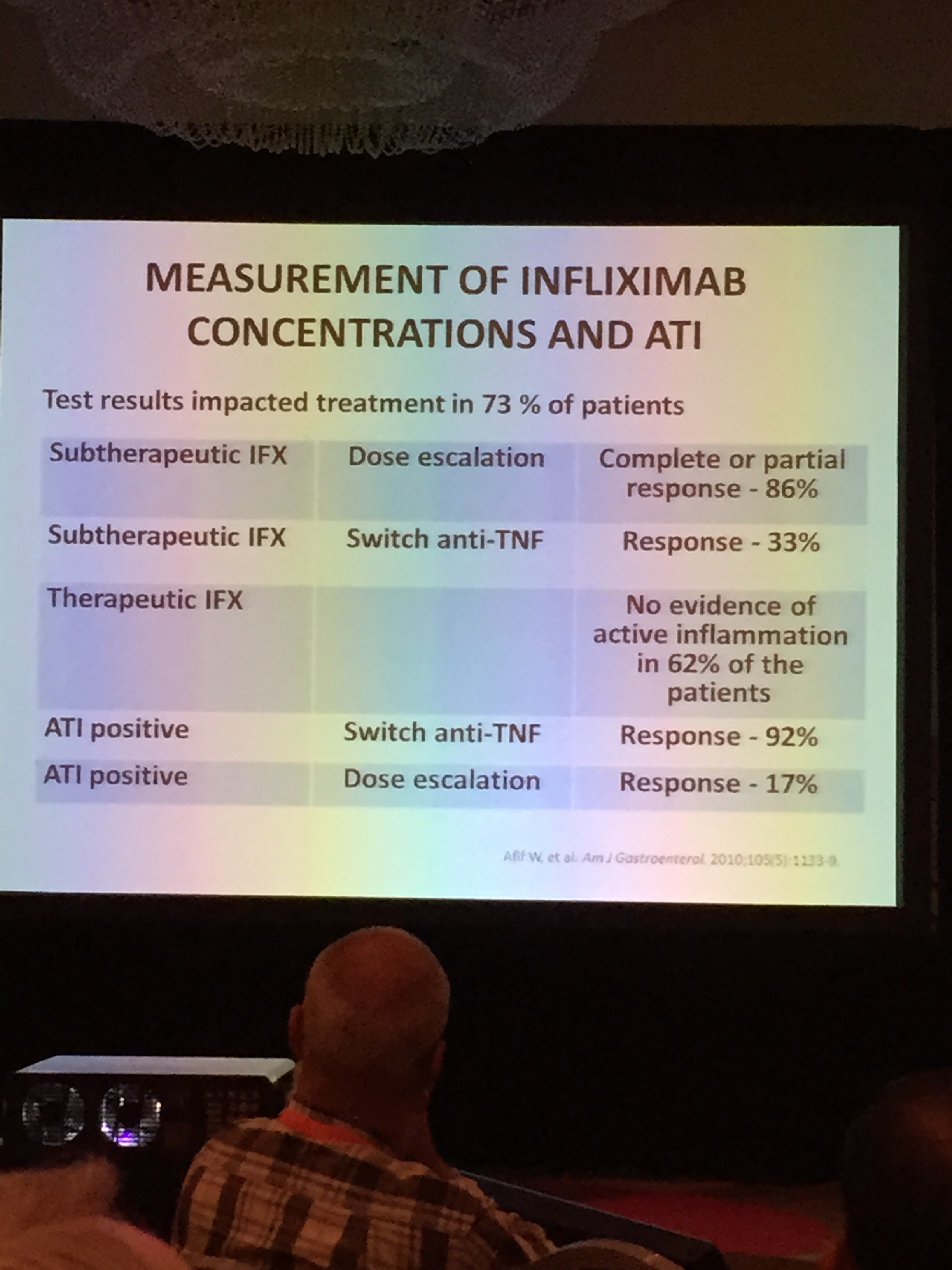
IFX Algorithm
- If losing response to therapy and if active disease is present, then check drug concentration. If subtherapeutic with no ADAs or low ADAs, dose escalation with or without immunomodulator is indicated.
- If subtherapeutic with high ADA, then change drug
- If therapeutic level, then may need to change to different anti-TNF or drug class.
Related posts on this topic:
- What you might not know about anti-TNF monitoring …
- Treating Allergic Reactions to Infliximab | gutsandgrowth
- Drug levels for inflammatory bowel disease | gutsandgrowth
- More Lessons in TNF Therapy (Part 2) | gutsandgrowth
- Monitoring TNF antagonists in inflammatory bowel disease …
Debate: Immunomodulators versus Biologic agents
- James Markowitz –consider starting with immunomodulators
- Maria Oliva-Hemker –consider starting with biologics
In the face of the “Biologic Tsunami,” Dr. Markowitz suggested –“Don’t throw the baby out with the bathwater”
- Reviewed infliximab data, and adalimumab data. 1-year remission rates 50-60%.
- Durability of infliximab may be influence by immunomodulators (IMs): patients who had IM prior to IFX had better durability of response: 45% durability in those who had no IM prior to biologic, 53% durability in those who had IM for ❤ months, 66% durability in those who had IM for >6 months prior to IFX.
- Adult data showing lack of efficacy with IMs influenced by different characteristics compared with children (eg. different disease location, ~40-50% of adults were smokers)
- Reviewed toxicity of IMs and biologics
- Children with severe disease do best with “early infliximab.”
- IMs with 40-60% efficacy over 18 months and then relatively stable.
- In Dr. Markowitz’ practice, IM use: girls receive thiopurines and boys receive methotrexate
Biologics –important to start before disease phenotype changed to stricturing/penetrating disease. (See images below)
Related posts:
- Superiority of Anti-TNF Therapy in Children | gutsandgrowth
- Superiority of Anti-TNF Therapy (Part 2) | gutsandgrowth
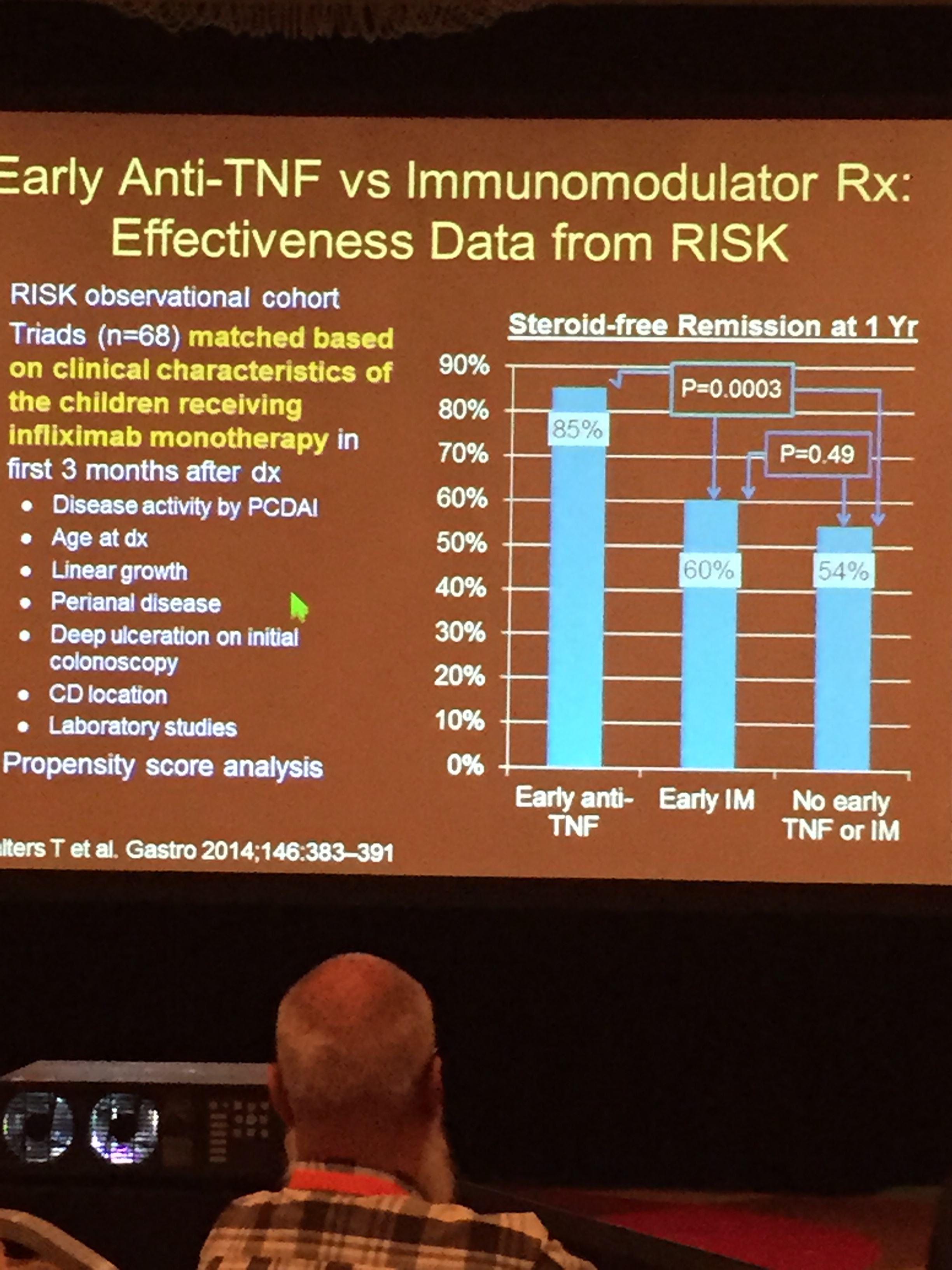
Early anti-TNF -RISK Cohort
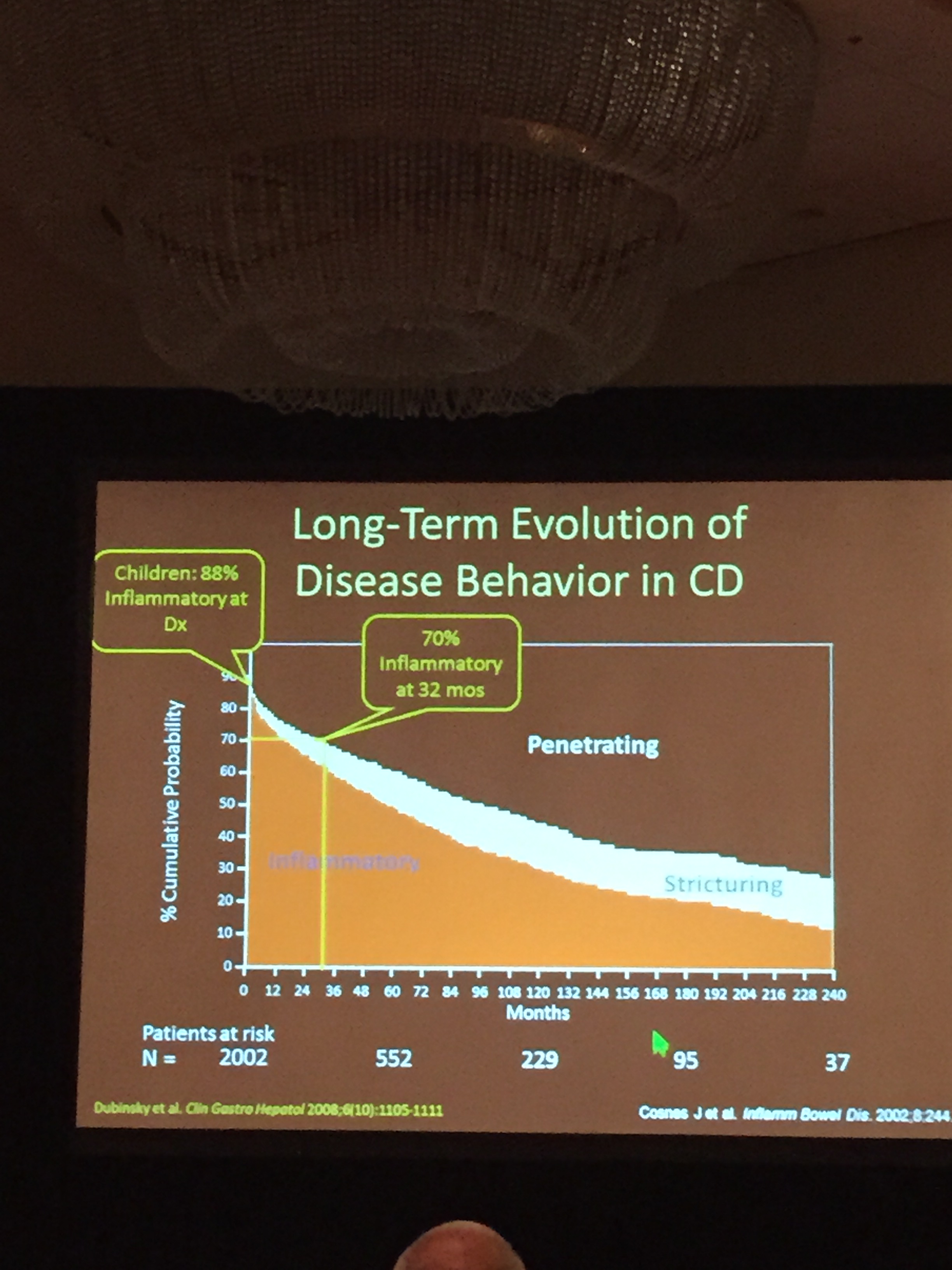
Long Term Risk of Stricturing (Cosnes et al)

Excellent summaries Jay. However would consider using MTX as adjuvant to lessen antibodies when therapeutic or sub IFX level and low level antibodies and then repeat levels. May lessen burning through IFX since remission rate on 2nd TNF is only 17%.
Sent from my iPhone
>
Pingback: What We Know Now: Therapeutic Drug Monitoring for Inflammatory Bowel Disease | gutsandgrowth
Pingback: Short Takes on IBD Articles | gutsandgrowth
Pingback: Toronto Consensus: Practice Guidelines for Nonhospitalized Ulcerative Colitis | gutsandgrowth
Pingback: PCDAI -Not Good Enough | gutsandgrowth
Pingback: New Target Drug Levels in Inflammatory Bowel Disease | gutsandgrowth
Pingback: Immune-Mediated Reactions to Anti-TNFs and What to Do About Them | gutsandgrowth
Pingback: How High Can You Go with Adalimumab? | gutsandgrowth
Pingback: Another Look at “Step-up” IBD Therapy | gutsandgrowth
Pingback: Support for Step-Up Therapy and Thiopurines | gutsandgrowth
Pingback: Safety of Long-term Adalimumab in Pediatrics; Weighted PCDAI | gutsandgrowth
Pingback: Adjustment of azathioprine dose in NUDT15 intermediate metabolizers, COVID-19 in Georgia & COVID-19 Phase 1 Vaccine Study | gutsandgrowth