

My wife has been receiving a lot of compliments for her daily jokes which she decided to post for all of the neighborhood walkers. “A lot of people cry when they cut an onion. The trick is not to form an emotional bond.”
This coronavirus disease has caused incredible upheaval & misery throughout the world. In addition, it has created an “infodemic.” This blog post is intended to collate my previous related posts/& many of the referenced links into one location, to provide GI society guidelines for PPE/endoscopy as well as to place a good image at the bottom:
- COVID-19 Projections -IHME Data IHME Link: IHME Website for COVID-19 This post details the projected needs (ventilators, ICU beds) and projected mortality. Currently, peak of this pandemic in U.S. is anticipated to be April 16th.
- How to Do a Colonoscopic Polypectomy and U.S. COVID-19 Tracker NPR: Map: Tracking The Spread Of The Coronavirus In The U.S This tracker details the pandemic in every state.
- How to Protect Healthcare Workers from COVID-19 -Lessons from Hong Kong and Singapore Atul Gawande has a very pertinent article in the New Yorker: Keeping the Coronavirus from Infecting Health-Care Workers
- What is the Current Standard of Care for PPE and Endoscopy Cases? Link to manuscript: COVID-19 in Endoscopy: Time to do more?
- Bill Gates: What We Need to Do Now for COVID-19, False-negative testing & Article Describing 3 Stages of Infection From NY Times: If You Have Coronavirus Symptoms, Assume You Have the Illness, Even if You Test Negative Bill Gates: Here’s how to make up for lost time on covid-19 & article describing 3 stages of infection: COVD-19 Illness in Native and Immunosuppressed States: A Clinical-Therapeutic Staging Proposal
- Allocating Scarce Resources During COVID-19 Pandemic Links CDC Link: Testing for COVID-19 Full Link NEJM 2020 (Ezekial J Emmanuel et al): Fair Allocation of Scarce Medical Resources in the Time of Covid-19. This post also displays some data on sensitivity/specificity of testing
- Iron Injectables Links Financial Times: Coronavirus tracked: the latest figures as the pandemic spreads | Free to read & from Johns Hopkins: COVID19 Caseload & Outcomes Worldwide
- COVID-19: Veneto vs. Lombardy and Georgia’s Part of this Pandemic Link: Harvard Business Review: Lessons from Italy’s Response to Coronavirus & Georgia DPH: COVID-19 Daily Status Report
- “Crushing It” Two More Pediatric Hepatitis C studies Full link from NY Times: How Long Will Coronavirus Live on Surfaces or in the Air Around You? and blog post shows how to properly place PPE
- Ethical Dilemmas and Digestive Symptoms –Common with COVID-19 Full link: NEJM: Facing Covid-19 in Italy — Ethics, Logistics, and Therapeutics on the Epidemic’s Front Line & digestive symptoms ACG: Full Link: ACG Media Statement
- More Advice on Coronavirus for Pediatric GIs: NASPGHAN and CCFA CCFA Guidance for Pediatric Caregivers and Patients —Updates on COVID-19 and IBD
- Autoimmune Hepatitis Outcomes, Grand Rounds on Splenomegaly, Hydroxychloroquine for SARS-CoV-2 & Zantac Warning
- Liver Shorts and COVID-19 Screenshots This post includes Fauci donuts, AJG reference on COVID-19 digestive symptoms, and technology to sterilized used PPE
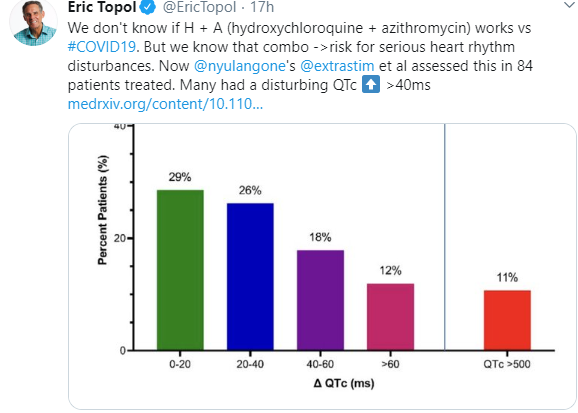
- New: NEJM link to video demonstrating need for PPE during intubation -see picture at bottom of post. Fluorescent Spray During Intubation and at the bottom -there is an image showing how hydroxychloroquine and azithromycin could increase risk for life-threatening arrhythmias
Aslo, recommendations from GI societies -AGA, ACG, ASGE and AASLD
- Use of Personal Protective Equipment in GI Endoscopy
- Endoscopic Procedure Guidance
JOINT GASTROENTEROLOGY SOCIETY MESSAGE: COVID-19
Use of Personal Protective Equipment in GI Endoscopy
RECOMMENDATIONS:
- General measures of physical distancing and adequate hand hygiene are of critical importance and need to be practiced diligently, independent of other protective measures.
- All elective, non-urgent procedures should be postponed until ample supplies of PPE, hospital beds and other resources are available after the COVID-19 surge.
- All members of the endoscopy team should wear a full set of PPE, predicated on resource availabilities.
- The correct sequence of putting on and taking off PPE (“donning” and “doffing”) is critical and needs to be understood and practiced [17].
- All members of the endoscopy team should wear N95 respirators (or devices with equivalent or higher filtration rates) for all GI procedures performed on patients with known SARS-CoV-2 infection and those with high risk of exposure. Given the high rate of infection transmission from pre-symptomatic individuals, all patients undergoing GI endoscopy in an area of community spread need to be considered ‘high risk’.
- All healthcare workers should have their N95 respirators fitted by an occupational health specialist prior to the first usage.
- Staffing of endoscopy rooms should be reduced to the minimum number of individuals necessary, in order to conserve PPE and other resources.
- In some cases, shortages may require extended and limited reuse of N95 respirators. Guidance is available on how to wear, remove and store respirators to minimize contamination [18]. Decontamination of N95 respirators with hydrogen peroxide vapor has been approved by the FDA as a means of reuse in times of limited supply [19].
|
|
Urgent/Emergent Procedures Should Not Be Delayed
- Upper and lower GI bleeding or suspected bleeding leading to symptoms
- Dysphagia significantly impacting oral intake (including EGD for intolerance of secretions due to foreign body impaction or malignancy (stent placement))
- Cholangitis or impeding cholangitis (perform ERCP)
- Symptomatic pancreaticobiliary disease (perform EUS drainage procedure if necessary for necrotizing pancreatitis and non-surgical cholecystitis, if patient fails antibiotics)
- Palliation of GI obstruction [UGI, LGI (including stent placement for large bowel obstruction) and pancreaticobiliary]
- Patients with a time-sensitive diagnosis (evaluation/surveillance/treatment of premalignant or malignant conditions, staging malignancy prior to chemotherapy or surgery)
- Cases where endoscopic procedure will urgently change management (e.g., IBD)
- Exceptional cases will require evaluation and approval by local leadership on a case by case basis
Q. Should all emergent EGD patients be intubated?
A. Absent other reasons that present a threat to the airway, intubation is not indicated for all EGDs. Proper use of PPE, including N95 masks is paramount.
Q. Should procedures be performed on patients with intermediate level cases such as Iron Deficiency Anemia (IDA) or mild dysphagia?
A. Decisions regarding cases such as these will need to be made on a case by case basis, taking into account resource availability, level of community infectivity and risk to the patient.


Pingback: NY Times: How Will We Know When to Reopen the Country? & Timely Tweets | gutsandgrowth
Pingback: High Risk Workers Need N95 Masks | gutsandgrowth
Pingback: NY Times: Japan’s Secret Success with Coronavirus | gutsandgrowth
Pingback: Eight States with Increasing COVID-19 Problems | gutsandgrowth
Pingback: 1st Cases of COVID-19 in Pediatric Inflammatory Bowel Disease –All Mild | gutsandgrowth
Pingback: Pandemic Is NOT Taking a Summer Holiday | gutsandgrowth
Pingback: Published IBD-COVID-19 Data from SECURE-IBD & Others | gutsandgrowth