
Two recent large studies examined the use of Upadacitinib, an oral JAK1 inhibitor, for Crohn’s disease and for Ulcerative Colitis.
- WJ Sandborn et al. Gastroenterology 2020; 158: 2123-38. Full text PDF: Efficacy and Safety of Upadacitinib in a Randomized Trial of Patients with Crohn’s Disease
- WJ Sandborn et al. Gastroenterol 2020; 158: 2139-49. Full text PDF: Efficacy of Upadacitinib in a Randomized Trial of Patients with Active Ulcerative Colitis
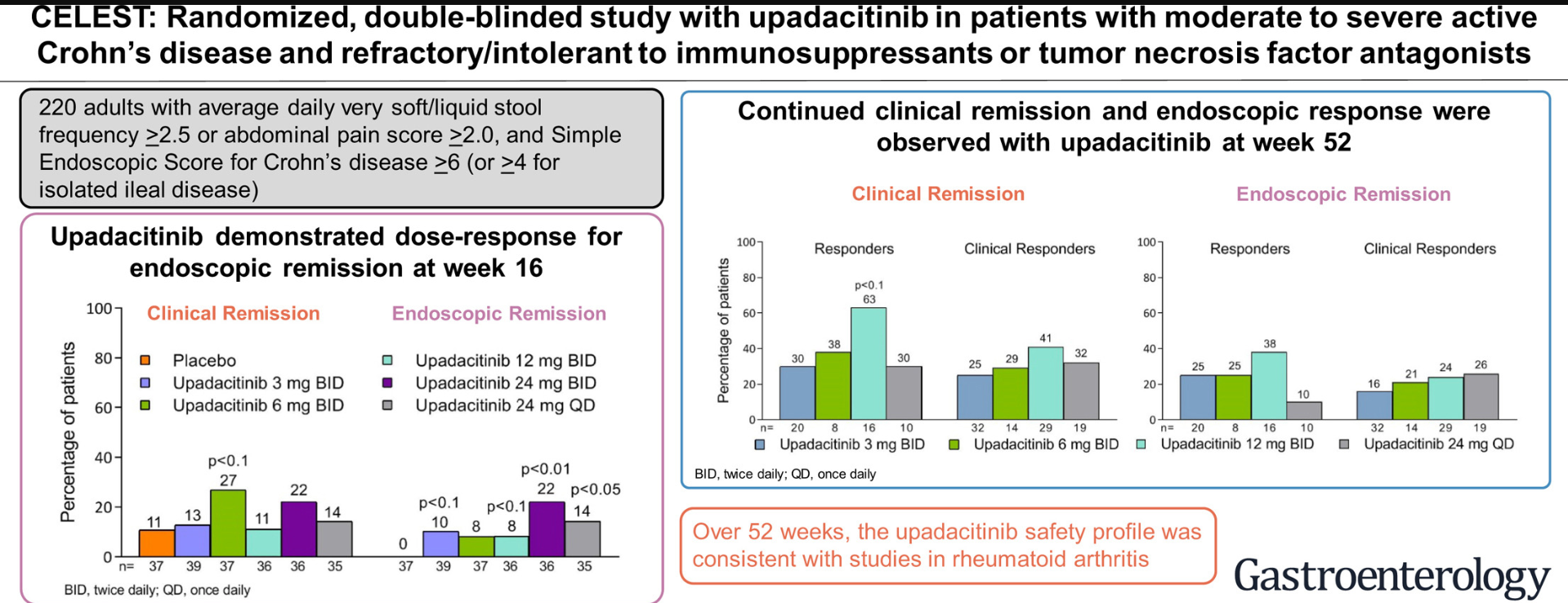
The first study, “CELEST,” (n=220) is the “first to evaluate the efficacy, safety, pharmacokinetics, and dose-response of upadacitinib immediate-release formulation in patients with moderate to severe CD and refractory to TNF antagonist therapy using PRO-based clinical and endoscopic endpoints… Nearly half of the patients enrolled in CELEST (44% [96/220]) were taking oral corticosteroids at baseline and underwent a mandatory taper starting at week 2.” The key findings are noted in the graphical abstract (below). A couple of additional points:
- During the induction period, the 24-mg twice-daily dose exhibited the most consistent association with meaningful improvements for multiple clinical and endoscopic endpoints at week 12 or 16
- Clinical remission was achieved by 13% of patients receiving 3 mg upadacitinib, 27% of patients receiving 6 mg upadacitinib (P < .1 vs placebo), 11% of patients receiving 12 mg upadacitinib, and 22% of patients receiving 24 mg upadacitinib
twice daily, and by 14% of patients receiving 24 mg upadacitinib once daily, vs 11% of patients receiving placebo. - Endoscopic remission was achieved by 10% (in 3 mg group) (P < .1 vs placebo), 8% (in 6 mg and 12 mg groups) (P < .1 vs placebo), 22% (in 24 mg BID group) (P < .01 vs placebo), and 14% (in 24 mg QD group) (P < .05 vs placebo) of patients receiving upadacitinib, respectively, vs none of the patients receiving placebo
- Upadacitinib was also associated with improvements in quality of life, based on IBDQ, observed as early as week 8
- AEs reported in this study were consistent with those previously observed in clinical trials with JAK inhibitors. Two patients had myocardial infarction events and 1 patient had a mesenteric vein thrombosis.
- Limitations: sample size, lack of placebo control during maintenance
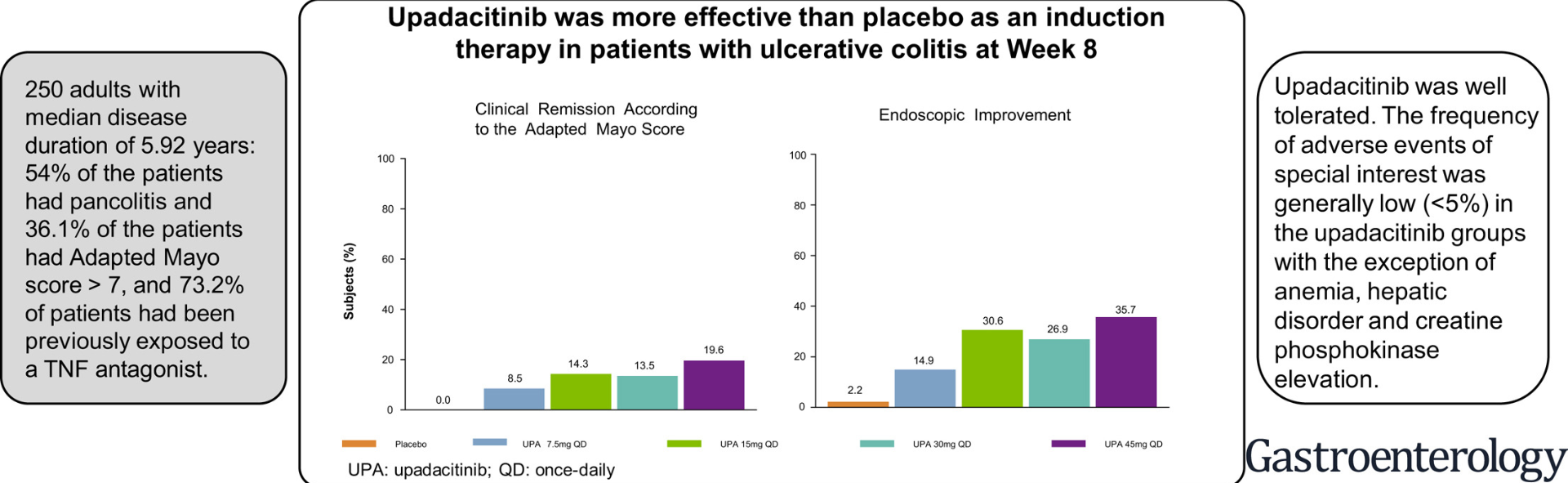
The second study, “U-ACHIEVE,” for ulcerative colitis (n=250) notes that in cellular assays upadacitinib is up to 60-fold selective for JAK1 over JAK2 and >100-fold selective over JAK3. The study incorporated a new definition for the primary endpoint of clinical remission using the adapted Mayo score with a more stringent criterion than previous studies. A consistent dose-response relationship with upadacitinib for this primary endpoint was observed. Other points:
- Upadacitinib was more effective than placebo for inducing remission in patients with moderately to severely active ulcerative colitis
- The onset of action was rapid, as shown by improvement in the partial
Mayo score at week 2 - Endoscopic improvement at week 8, defined as endoscopic subscore of 1, was achieved in 14.9%, 30.6%, 26.9%, and 35.7% of patients receiving upadacitinib 7.5 mg, 15 mg, 30 mg, or 45 mg, respectively, compared with 2.2% receiving placebo (P ¼ .033, P < .001, P < .001, and P < .001 compared with placebo, respectively)
- Histologic improvement was demonstrated in all treatment arms
- The types of AEs reported in this study were similar to those previously observed in clinical trials with JAK inhibitors. In the 45 mg daily arm, one patient developed herpes zoster and one participant developed deep venous thrombosis/pulmonary embolism (26 days after discontinuation of study medication)
My take: Upadacitinib looks quite promising for ulcerative colitis and is likely to be helpful in a smaller subset of patients with Crohn’s disease. HIgher doses appear to be more effective but are likely to be associated with higher rates of adverse events. Further studies, including pediatric trials, are needed.
