
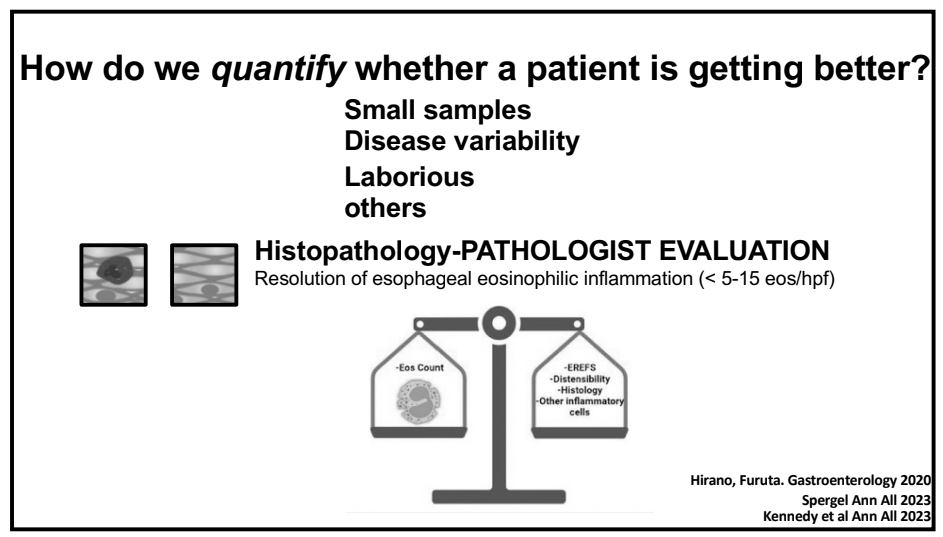
We recently had Glenn Furuta, MD give our group a terrific lecture on eosinophilic esophagitis (EoE).
Some of the key points:
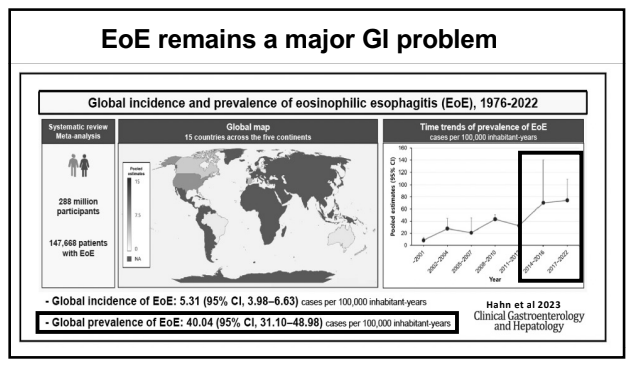
- The burden of EoE continues to increase.
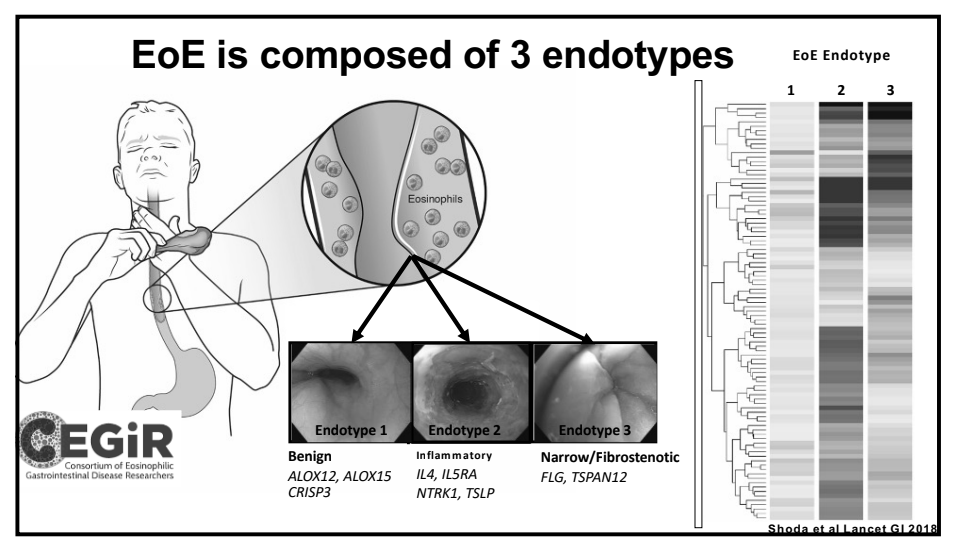
- There are clearly several phenotypes of EoE. Some patients may never develop stricturing/fibrostenotic disease but natural history data continues to evolve.
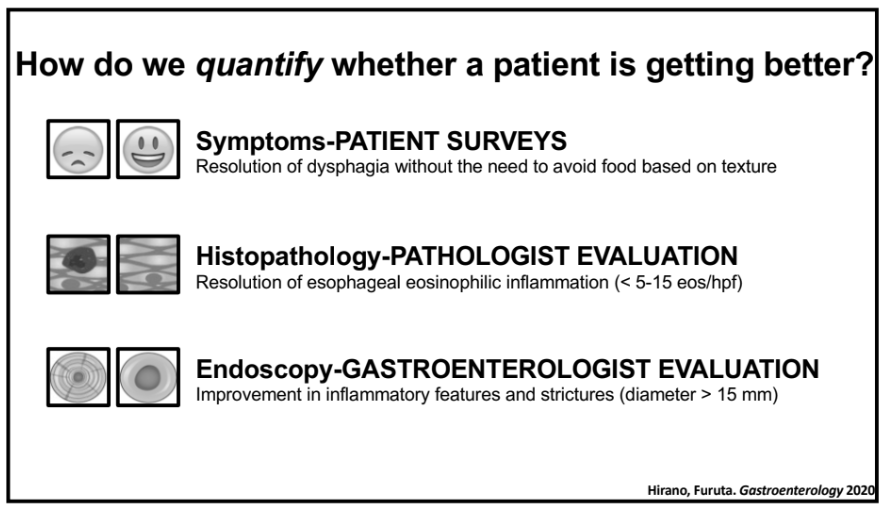
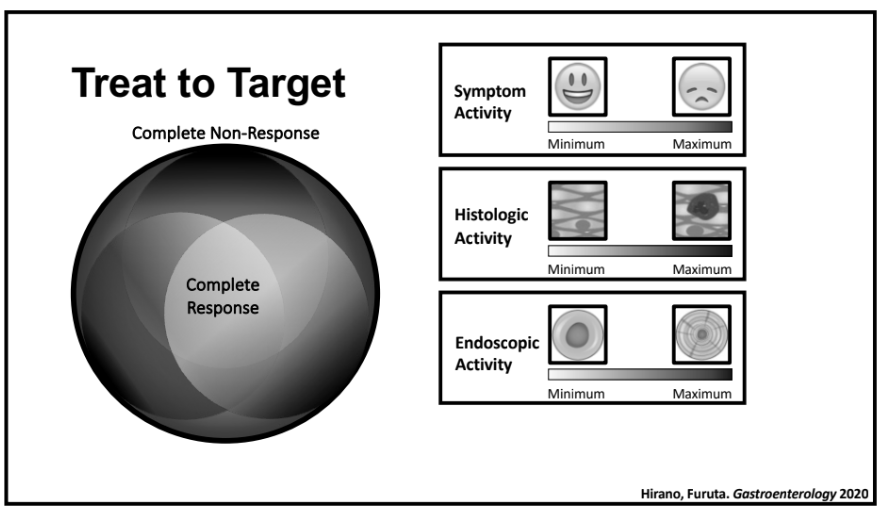
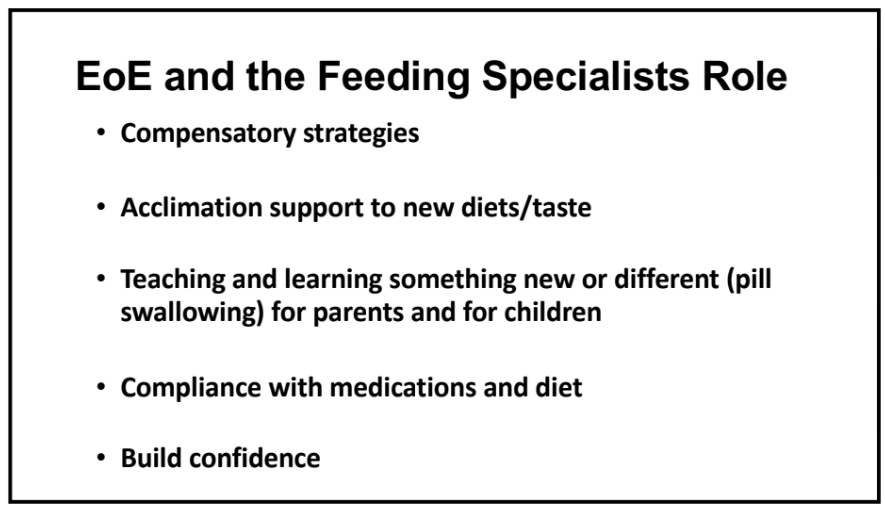
- After treatment response, many patients can continue with symptoms. In adults and adolescents, this has been termed ‘esophageal hypervigilance.’ Feeding therapy may be helpful in this circumstance.
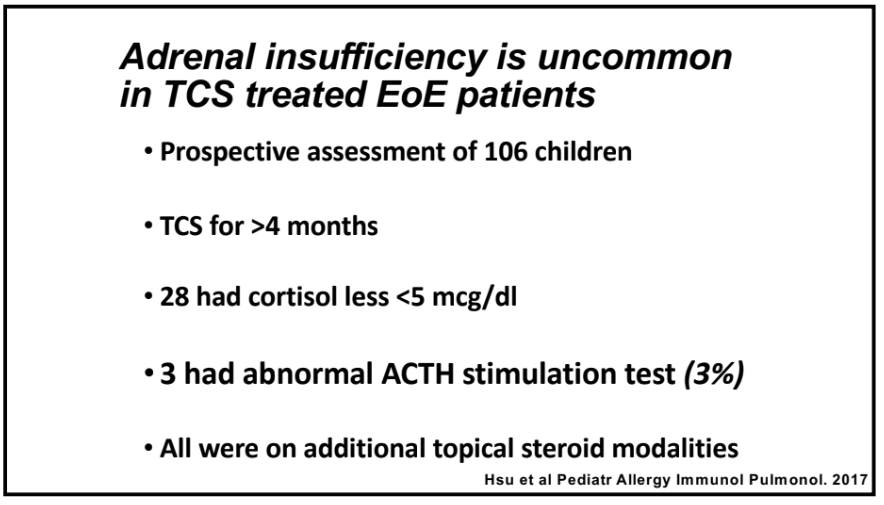
- Adrenal insufficiency: Currently their group tries to screen for this after 4 months of topical corticosteroids and then yearly. It is unusual for them identify adrenal insufficiency if the patient is receiving only a single steroid agent; patients receiving steroids for other conditions like asthma are at higher risk.
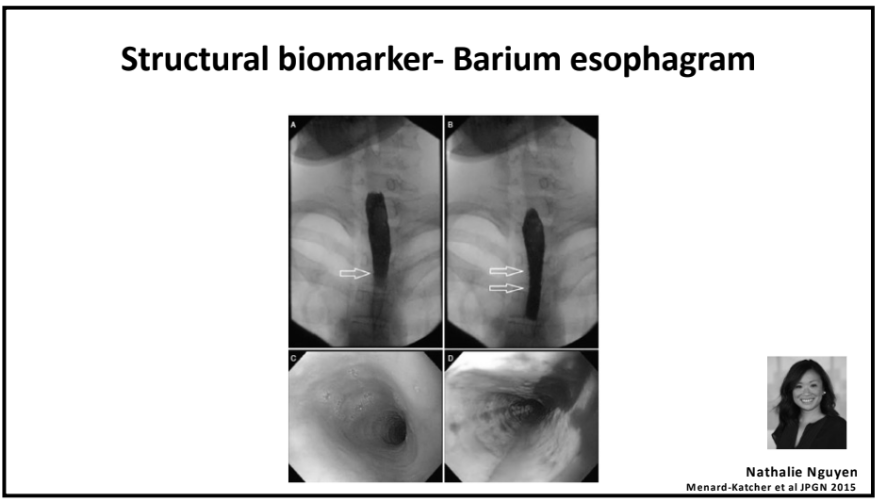
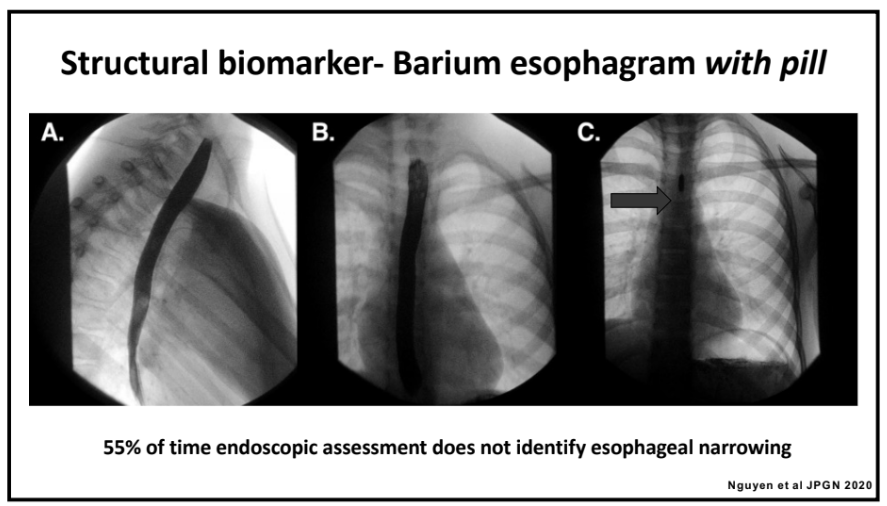
- An esophagram with a barium coated pill can be a useful adjunct to determine if there is esophageal narrowing (this can be missed on endoscopy).
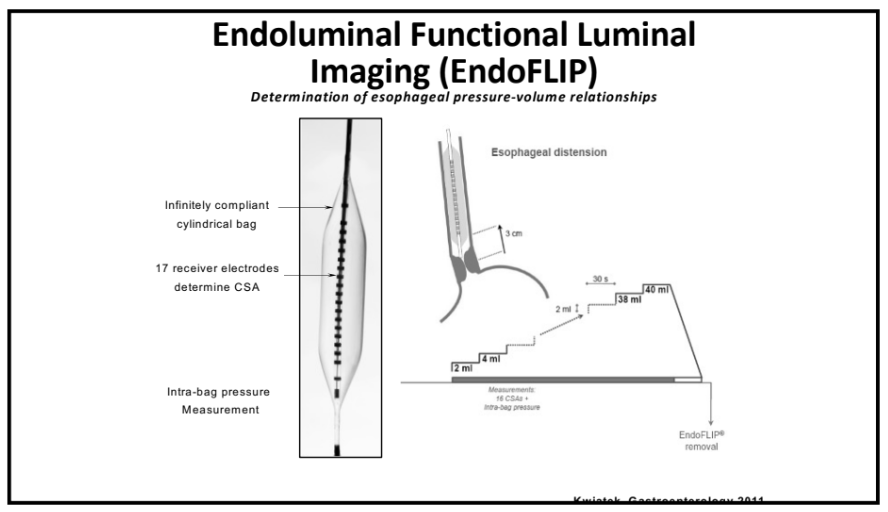
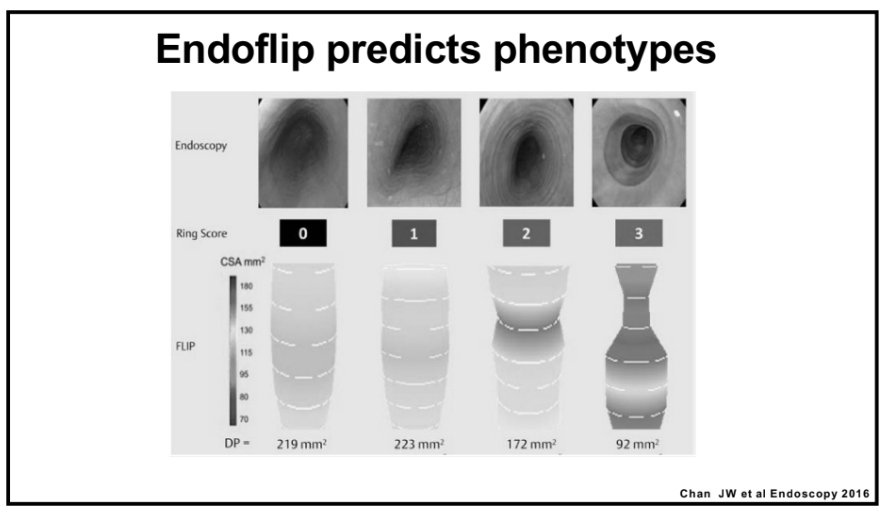
- For select patients, endoFLIP can characterize distensibility/esophageal function
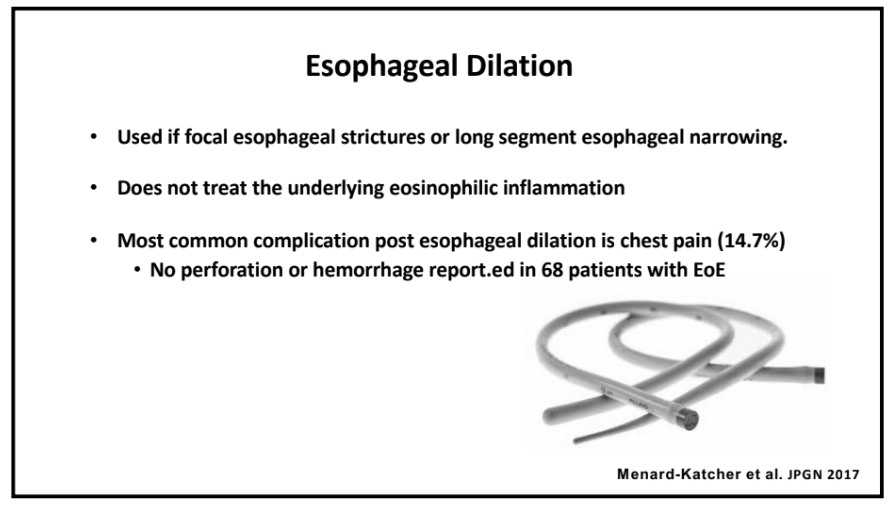
- Esophageal strictures: Their group uses Bougie dilators and has had a good experience. No perforations. ~15% with chest pain afterwards.
- Corticosteroids (topical) can reduce the risk of food impactions in adults.
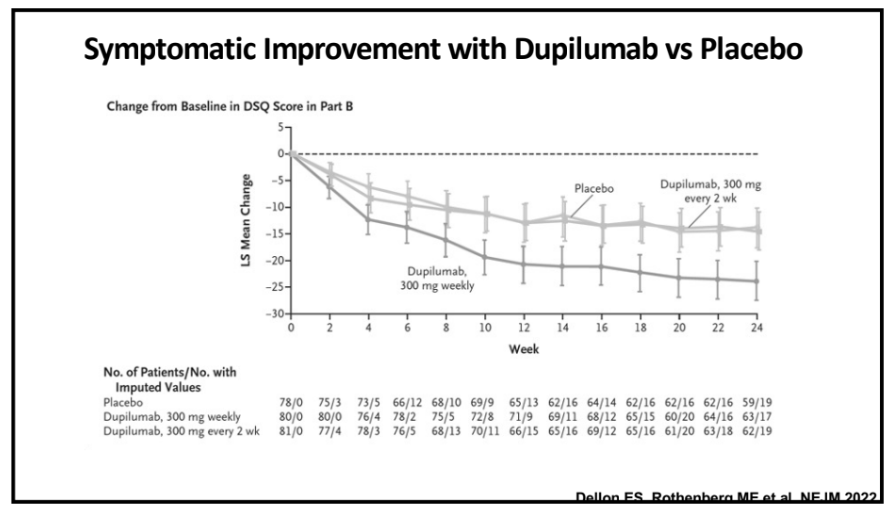
- Reviewed use of Dupilimab and its recent approval in EoE for children as young as 1 yr of age (>15 kg)
Some selected slides:





Related blog posts:
- Dupixent Approved in Younger Children (15 kg+)
- Eosinophilic Esophagitis -Increasing Incidence and Emergence of Biologic Treatments
- NASPGHAN YouTube Video for Eosinophilic Esophagitis
- Increasing Burden of Eosinophilic Esophagitis
- FLIP Patterns for Adults with Eosinophilic Esophagitis
- But How Well Does It Work in Theory and Eosinophilic Esophagitis Treatments
- Practical Guide to Dietary Therapy for Eosinophilic Esophagitis
- When to Use Dupilumab for Eosinophilic Esophagitis: Multispecialty Guidelines
- Managing Adrenal Insufficiency in Eosinophilic Esophagitis
- Landmark Dupilumab Study for Eosinophilic Esophagitis
- Dupilumab: FDA Approval for Eosinophilic Esophagitis
