
R Panaccione et al. Clin Gastroenterol Hepatol 2026; 24: 1424-1433. Open Access! Impact of Extended Risankizumab Treatment in Patients With Ulcerative Colitis Who Did Not Respond to Induction Treatment
Methods:
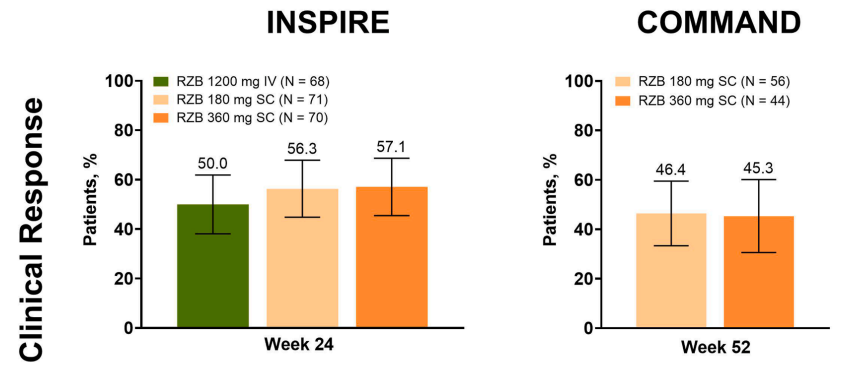
- In the AbbVie-funded phase 3 INSPIRE induction study, 209 initial nonresponders to 12 weeks of 1200 mg intravenous (IV) risankizumab induction were rerandomized to receive 12 weeks of additional 1200 mg risankizumab (weeks 12, 16, and 20) or 180 mg or 360 mg subcutaneous [SC] risankizumab (weeks 12 and 20) in a double-blind fashion
- Then, the delayed responders continued to receive blinded risankizumab at their assigned dose in the phase 3 COMMAND maintenance study
- Clinical response per adapted Mayo Score (AMS): decrease from baseline ≥2 points and ≥30% from baseline, plus a decrease in RBS ≥1 or an absolute RBS ≤1
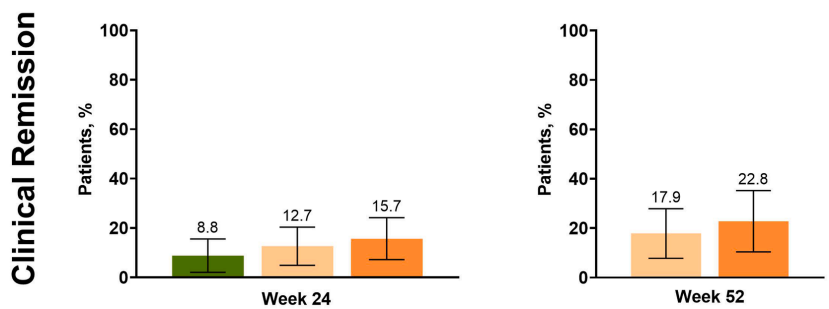
- Clinical remission per AMS: SFS ≤1 and not greater than baseline, RBS = 0, and endoscopic subscore ≤1 without the evidence of friability
Key findings:
- Initial nonresponders (1200 mg IV [n = 68], 180 mg SC [n = 71], or 360 mg SC [n = 70]) had week 24 clinical response rates of 50%, 56.3%, and 57.1%, respectively
- Patients also achieved clinical remission, histologic endoscopic mucosal improvement (8.8%, 12.7%, and 15.7% for both endpoints), endoscopic improvement (17.6%, 18.3%, and 24.3%), and endoscopic remission (1.5%, 8.5%, and 5.7%)
My take: A longer trial of risankizumab is often needed to know with certainty if it will work for ulcerative colitis. More than half of initial nonresponders acquire a clinical response with extended therapy. A similar pattern was noted for risankizumab with Crohn’s disease.
Related blog post: Over 60% of Initial Nonresponders Improve with Extended Risankizumab Therapy for Crohn’s Disease
