
C DiLorenzo, M Saps et al. Gastroenterol 2026; 170: 1367-1387. Open Access! Lower and Biliary Disorders of Gut–Brain Interaction: Child and Adolescent
Yesterday’s post reviewed DGBIs related to the lower GI tract causing either abdominal pain or discomfort disorders. Today’s post focuses on DGBIS related to Defecation and Anorectal Disorders.
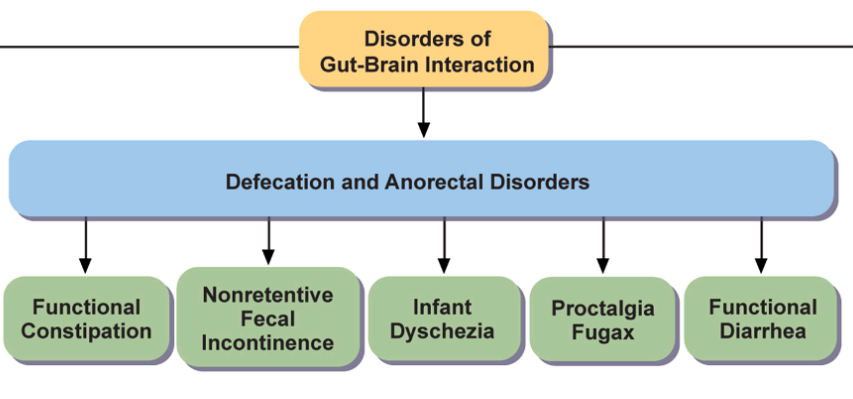
Functional Constipation
- “The committee debated whether it was beneficial to remove the term “functional” from this entity to maintain uniformity with other DGBI. It was concluded that there was no better alternative to describe this condition.” (JH: ??dysfunctional)
- “There is evidence that abdominal radiographs are neither sensitive nor specific to diagnose FC so they should only be used when clinically indicated. However, a moderate to large amount of stool found in the rectum has a high sensitivity and positive predictive value (>80%) for fecal retention as assessed by abdominal radiograph.132“
- Treatment should include adequate fiber and fluid intake. “Regarding maintenance [medication] therapy, the ESPGHAN-NASPGHAN guidelines recommend polyethylene glycol as the first-line therapy for children older than 6 months with constipation.139 In children not improving with stool softeners, adding a stimulant laxative, such as senna or bisacodyl, to the treatment may be beneficial.140 … [also] linaclotide… is now approved in the United States at the dosage of 72 μg/day in patients aged 6–17 years.141,142“
- “NASPGHAN defined refractory constipation as ongoing constipation in children who meet Rome IV Criteria for FC, who failed to improve after a minimum of 3 months of appropriate conventional therapies.”
- Related blog posts: Position Paper: Pediatric Refractory Constipation Management & Willie Sutton and Refractory Constipation
Nonretentive Fecal Incontinence
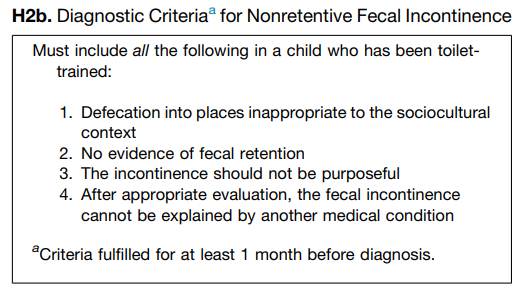
- “The word “functional” was removed to maintain consistency with the other DGBI. The Committee understands that the current definition does not capture the subset of children who have never been toilet-trained and have purposeful incontinence because of emotional or psychological issues…these children do not have a classic DGBI, and … exclude them from this definition by adding a statement that the incontinence should not be purposeful.”
- Psychology: “The pressure from peers and from family members due to the unpleasant odor is usually substantial. Thus, it is unsurprising that most children with this symptom have psychological problems, irrespective of what causes the incontinence.155,156 They also face significant risks of child maltreatment.154,155“
- Treatment: “Patients should be instructed to sit on the toilet for approximately 5–10 minutes with appropriate seating methods at least 3 times per day, especially when they return from school…One case report showed the efficacy of loperamide in treating children with NRFI.157 There is no benefit to treating children with NRFI with laxatives, which may worsen the symptoms.158 The use of fiber may be beneficial in certain cases.”
Infant Dyschezia
- Prevalence is estimated at 4-5% of all infants
- Treatment: “Caregivers are frequently reassured by a methodical physical examination. They usually accept the explanation that the child needs to learn to relax the pelvic floor at the same time as bearing down. The caregivers are advised to avoid rectal stimulation, which produces sensory experiences that may be noxious or that may condition the child to wait for stimulation before defecating. Laxatives are usually unnecessary.”
- Related blog post: Are There Any Babies with a Normal GI Tract?
Proctalgia Fugax
- “The pain in PF is characterized by a sudden onset of severe cramping or stabbing pain in the rectum that lasts from seconds to several minutes and disappears completely.”
- “Most children are managed with a simple explanation of the transient and benign nature of the disorder. Treatment is indicated in severe cases only. In adults, persistent symptoms can be treated with local application of 0.2% glyceryl trinitrate or 2% diltiazem at the onset of symptoms.169“
Functional Diarrhea
- “FDr is characterized by diarrhea without significant pain, whereas IBS-D presents with pain as the predominant symptom.”
- Evaluation: “Attention should be given to ruling out conditions such as celiac disease, inflammatory bowel disease, malabsorption syndromes (eg, sucrase–isomaltase deficiency), and infectious causes. The physical examination should specifically assess hydration, nutritional status, and alarm signs (Table 3).186,187 In most cases, the likelihood of an underlying organic disease can be reasonably excluded through basic bloodwork and stool tests.”
- Treatment: “Most toddlers and preschoolers do not require medical therapy. In older children, treatment depends on symptom severity and impact on quality of life…Dietary evaluation is recommended—especially reduction of juice and fructose intake in young children.188,189 A low-FODMAP diet may be trialed in older children. Other treatments include loperamide,79 bile acid sequestrants (eg, cholestyramine),78 and 5–hydroxytryptamine type 3 antagonists when symptoms are persistent.”
- Related blog post: AGA Guidelines for Evaluation of Functional Diarrhea and IBS-D
My take: Overall, the Rome V guidelines make a lot of incremental improvements.
