Thanks to Chelly Dykes for presenting poster later today and to co-authors for collaborating on this project: Jeffery Lewis, Bonney Reed-Knight and Cate Crenson.
Full abstract below.

ABSTRACT:
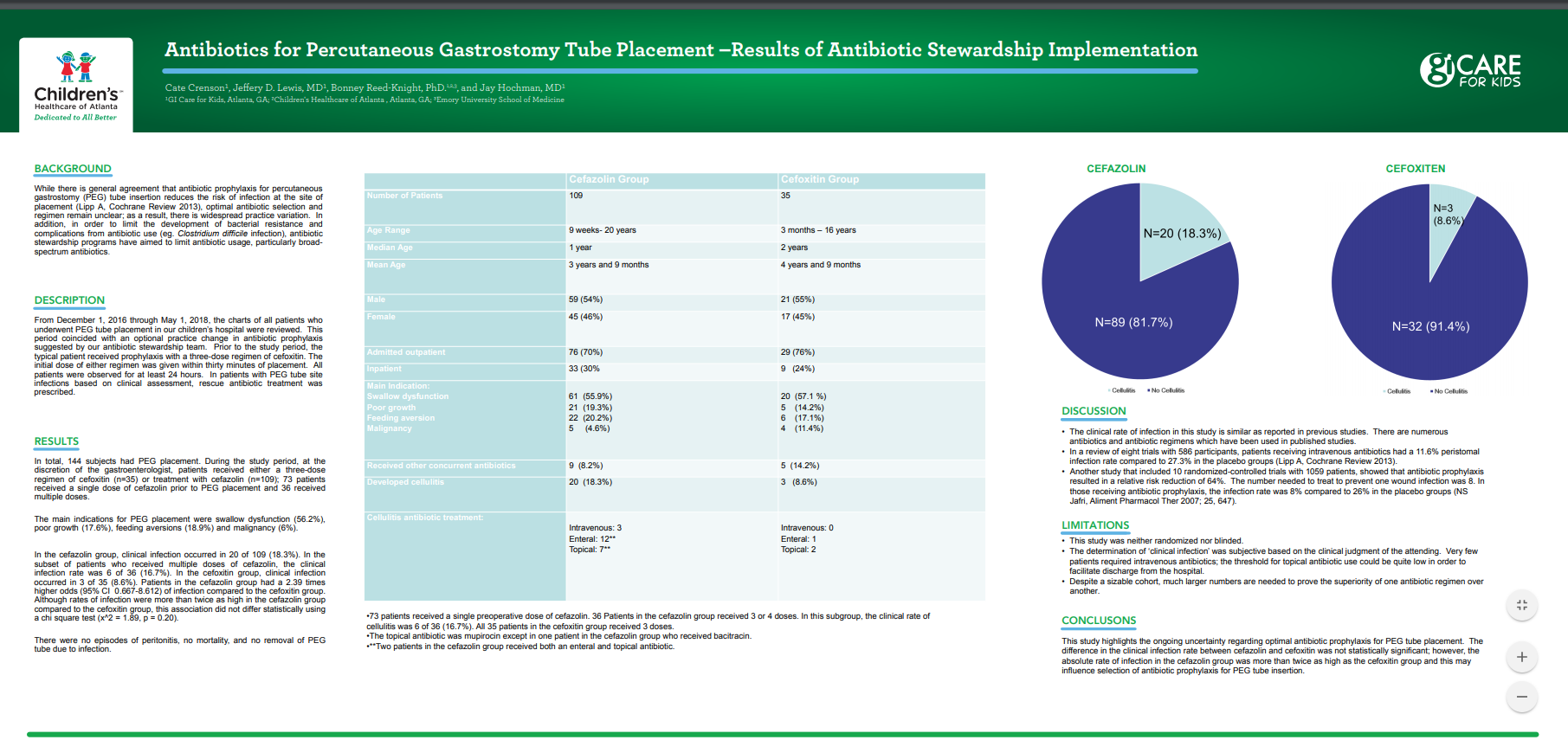
Background: While there is general agreement that antibiotic prophylaxis for percutaneous gastrostomy (PEG) tube insertion reduces the risk of infection at the site of placement (Lipp A, Cochrane Review 2013), optimal antibiotic selection and regimen remain unclear; as a result, there is widespread practice variation. In addition, in order to limit the development of bacterial resistance and complications from antibiotic use (eg. Clostridium difficile infection), antibiotic stewardship programs have aimed to limit antibiotic usage, particularly broad-spectrum antibiotics.
Methods: From December 1, 2016 through May 1, 2018, the charts of all patients who underwent PEG tube placement in our children’s hospital were reviewed. This period coincided with an optional practice change in antibiotic prophylaxis. Prior to the study period, the typical patient received prophylaxis with a three-dose regimen of cefoxitin. During the study period, at the discretion of the gastroenterologist, patients received either a three-dose regimen of cefoxitin (n=38) or treatment with cefazolin (n=109); 73 patients received a single dose of cefazolin prior to PEG placement and 36 received multiple doses. The initial dose of either regimen was given within thirty minutes of placement. All patients were observed for at least 24 hours. In patients with PEG tube site infections based on clinical assessment, rescue antibiotic treatment was prescribed.
Results: In total, 144 subjects had PEG placement. The main indications for PEG placement were swallow dysfunction (56.2%), poor growth (17.6%), feeding aversions (18.9%) and malignancy (6%). In the cefoxitin group, clinical infection occurred in 3 of 35 (8.6%). In the cefazolin group, clinical infection occurred in 20 of 109 (18.3%). In the subset of patients who received multiple doses of cefazolin, the clinical infection rate was 6 of 36 (16.7%). Patients in the cefazolin group had a 2.39 times higher odds (95% CI 0.667-8.612) of infection compared to the cefoxitin group. Although rates of infection were more than twice as high in the cefazolin group compared to the cefoxitin group, this association did not differ statistically using a chi square test (x^2 = 1.89, p = 0.20).
Conclusion: This study highlights the ongoing uncertainty regarding optimal antibiotic prophylaxis for PEG tube placement. The difference in the clinical infection rate between cefazolin and cefoxitin was not statistically significant; however, the absolute rate of infection in the cefazolin group was more than twice as high as the cefoxitin group and this may influence selection of antibiotic prophylaxis for PEG tube insertion.