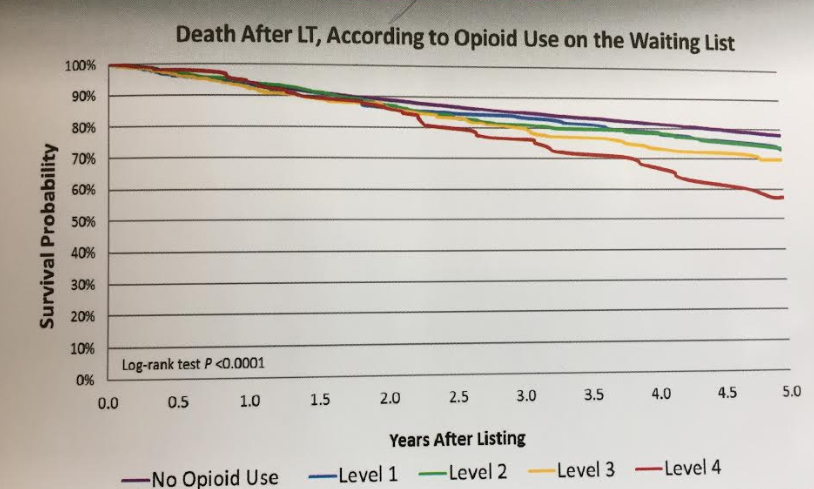
Not surprisingly, a recent study (HB Randall et al. Liver Transplantation 2017; 23: 305-14) has found that use of opioid medications prior to liver transplantation (LT) increased mortality over 5 years after transplantation.
This retrospective cohort study with data from nearly 30,000 patients correlated outcomes with pre-LT opioid exposure. Overall, 9.3% of recipients filled opioid prescriptions while on the waiting list. Adjusted hazard ratios for death were 1.28 and 1.52 respectively for opioid use of level 3 and level 4.

In the associated editorial (pg 285-7), the authors note that animal models have shown direct hepatotoxic effects of opioid use, though they speculate that the driver for mortality could be due to “sustained opioid use over time or return to illicit drug use.”
A unrelated commentary by CDC director Tom Frieden (AJC “Protect Ga. families from opioid overdose”, March 18, 2018) explains the scope of the opioid epidemic. “Since 2000, more than 300,000 of our sons, daughters, brothers, sisters, mothers, fathers, and friends have been killed by opiates. In 19999, approximately 6,000 Americans died from opiate overdose –including both prescription pain medicines … and heroin. By 2015 that number increased to more than 33,000.” This is more than a five-fold increase.
He emphasized that opiates serve as a gateway drug for those addicted to heroin; that is, the majority of those hooked on heroin were started on an opioid medication.
My take: The worsened outcomes of LT due to opioids are unfortunately a tiny part of an enormous tragic problem of the opioid epidemic.
Related posts: