
I am fortunate to work closely with several well-qualified pediatric surgeons and colorectal surgeons. When faced with perianal fistulas, I have discussions with them to help optimize therapy. Understanding exactly what and why the surgeons do what they do has not always been clear to me. Four recent articles provide guidelines for the management of Crohn’s perianal disease. The color figures in the articles make understanding what is done pretty obvious.
- Schwartz DA et al. Inflamm Bowel Dis 2015; 21: 723-30. Overview.
- Ong EMW et al. Inflamm Bowel Dis 2015; 21: 731-36. Focus on imaging.
- Schwartz DA et al. Inflamm Bowel Dis 2015; 21: 737-52. Critical evaluation of Medications
- Fichera A, Zoccali M. Inflamm Bowel Dis 2015; 21: 753-58. Critical evaluation of Surgical Approaches
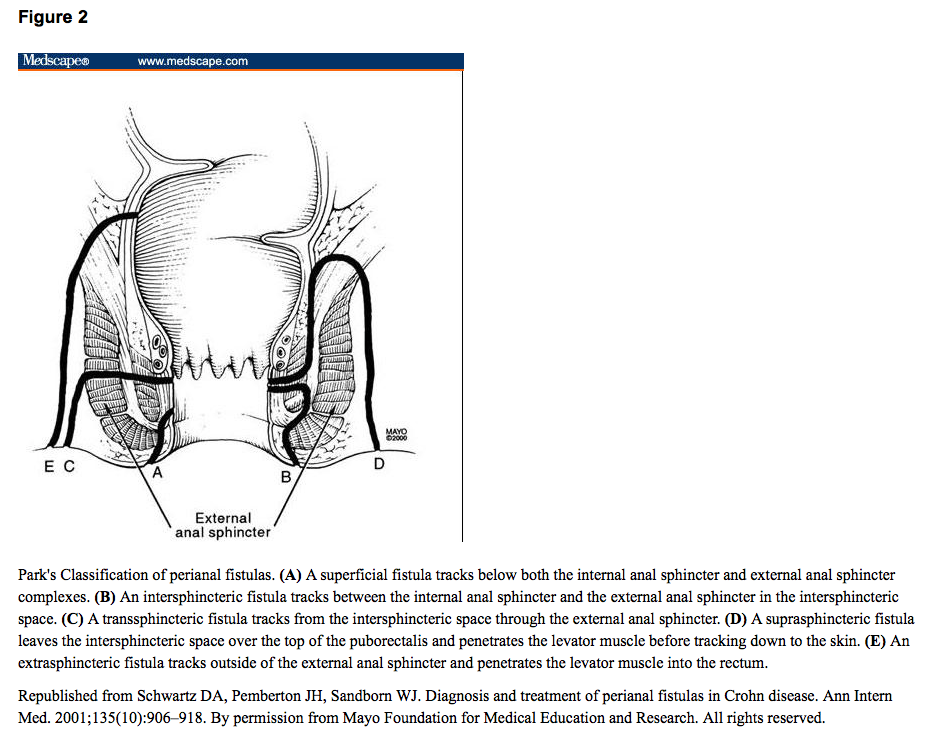
The first guideline provides a summary statement combining aspects of both medical and surgical management. Basic anatomy and classification are reviewed (a color figure similar to reproduction below helps describe the types of fistula).
Screenshot from Medscape: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1681560/
Simple vs Complex fistula is reviewed. A “Simple fistula is a superficial, intersphincteric or low transspincteric fistula that has only 1 opening and is not associated with an abscess and/or does not connect to an adjacent structure such as the vagina or bladder.” All others are complex fistulas. The MRI classifcation is also reviewed (Figure 5).
Other points:
- For fistulizing disease, top-down cotherapy (anti-TNF/immunomodulator) therapy is recommended. Antibiotics are recommended in the short term.
- Placement of a draining seton (for complex fistulas) helps to maintain fistula drainage until the track becomes inactive on medical treatment.
- A treatment algorithm (Figure 7) notes that endoscopy, imaging (EUS or MRI) and exam under anesthesia are key first steps. Decision tree then divides based on whether there is rectal inflammation, and whether fistula is simple or complex.
- Surgical options include fistulotomy, fibrin glue, fistula plug, seton placement, advancement flaps and proctectomy.
Bottomline: These set of articles should serve as a useful reference when managing perianal disease.
Related blog posts:
- Pediatric Consensus Statement: Perianal Crohn Disease …
- CCFA Conference Notes 2014 (part 2) | gutsandgrowth

Pingback: Fecal Diversion for Perianal Crohn’s Disease | gutsandgrowth
Pingback: Ileocecal Resection in Pediatric Crohn’s Disease | gutsandgrowth
Pingback: IBD Shorts and Postop Crohn’s Management | gutsandgrowth