MD Kappelman et al. Gastroenterology. 2023: 165: 149-161. Open Access! Comparative Effectiveness of Anti-TNF in Combination With Low-Dose Methotrexate vs Anti-TNF Monotherapy in Pediatric Crohn’s Disease: A Pragmatic Randomized Trial
This study enrolled 297 children with Crohn’s disease starting anti-TNF therapy. Patients initiating infliximab or adalimumab were randomized in 1:1 allocation to methotrexate or placebo and followed for 12–36 months.
Methotrexate dosing: For those in the active arm, oral methotrexate was administered with a weekly dose of 15 mg for children ≥40 kg, 12.5 mg for children 30 to <40 kg, and 10 mg for children 20 to <30 kg. All participants received pretreatment with ondansetron 4 mg (or placebo) to prevent nausea and folic acid (1 mg/d).
Key findings:
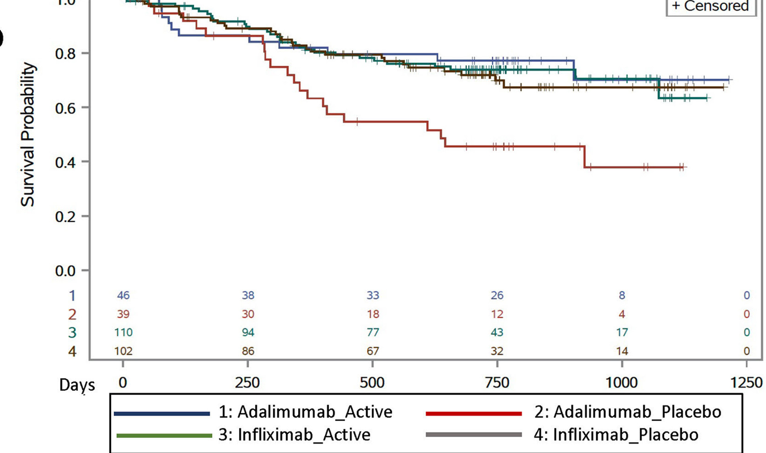
- For treatment failure: among infliximab initiators, there were no differences between combination and monotherapy (hazard ratio, 0.93; 95% CI, 0.55–1.56)
- For treatment failure: among adalimumab initiators, combination therapy was associated with longer time to treatment failure (hazard ratio, 0.40; 95% CI, 0.19–0.81).
- A trend toward lower anti-drug antibody development in the combination therapy arm was not significant (infliximab: odds ratio, 0.72; 95% CI, 0.49–1.07; adalimumab: odds ratio, 0.71; 95% CI, 0.24–2.07).
- In our study, only 38% of participants underwent colonoscopy during follow-up (41% had calprotectin measurement).
My thoughts on this study:
- The COMMIT study Gastroenterol 2014; 146: 681-88 found similar findings with regard to infliximab (see blog post: Digging into the COMMIT Study). In this study, MTX with IFX was not superior to monotherapy but did result in fewer antibodies and better levels.
- With IFX the benefits of combination therapy seem to be minimal in those with good therapeutic levels, S Lega et al. Inflamm Bowel Dis 2019; 25: 134-41, JF Colombel et al. Clin Gastroenterol Hepatol 2019; 17: 1525-32: (blog posts: Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy for IBD?; Combination Therapy Study Points to Central Role of Adequate Drug Levels). In the discussion, the authors note that intensive therapeutic drug monitoring may contribute to better outcomes with infliximab compared to adalimumab. “The observed benefit of combination therapy among adalimumab users was demonstrated in the setting of standard of care TDM. Of note, anti-TNF dose or interval adjustment and TDM were more frequent in infliximab-treated patients than adalimumab-treated patients, likely due to ease of obtaining trough levels during infusions and more flexible dosing.”
- In those on their 2nd anti-TNF, dual therapy is likely more important: NV Castelle et al. Clin Gastroenterol Hepatol 2022; 20: 465-467 (post: Low Anti-TNF Levels or Antibodies Are Associated with Antibodies to Subsequent Anti-TNF Agent)
My take: Given the increased difficulty monitoring the kids on adalimumab, they are probably better off on dual therapy. My suspicion, though, is that if they had optimized levels, the benefit of dual therapy is probably small and would mirror the findings with IFX.