
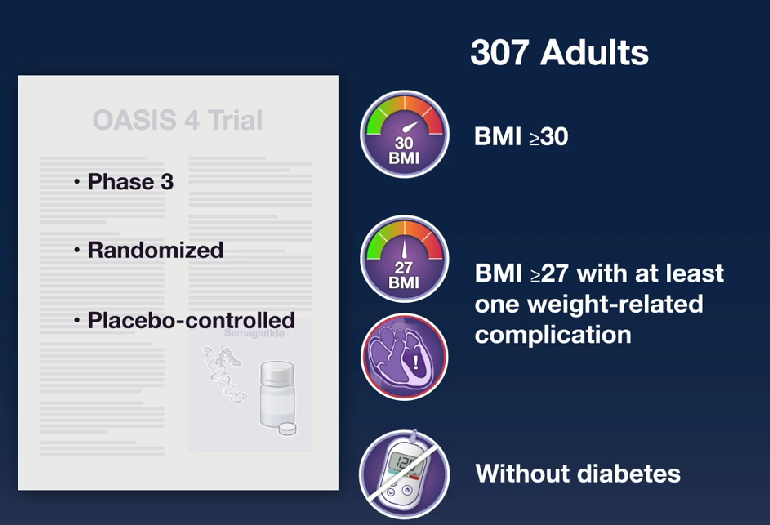
SWharton et al. N Engl J Med 2025;393:1077-1087. Oral Semaglutide at a Dose of 25 mg in Adults with Overweight or Obesity
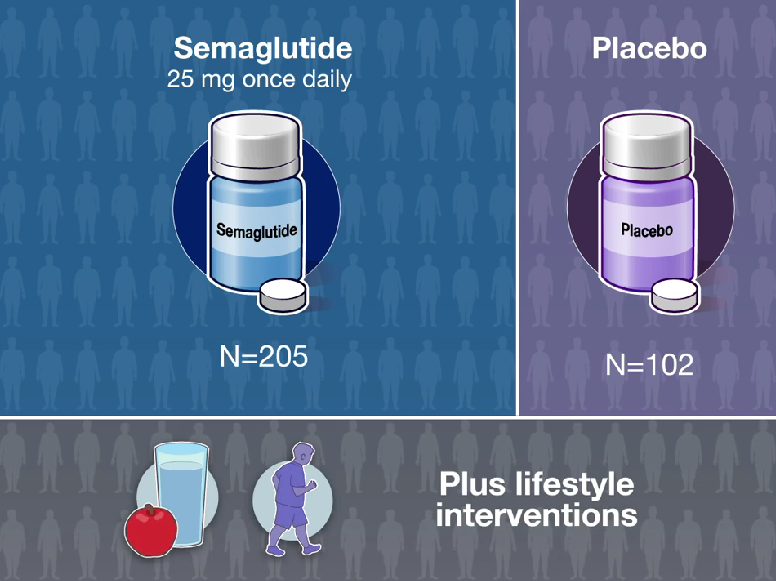
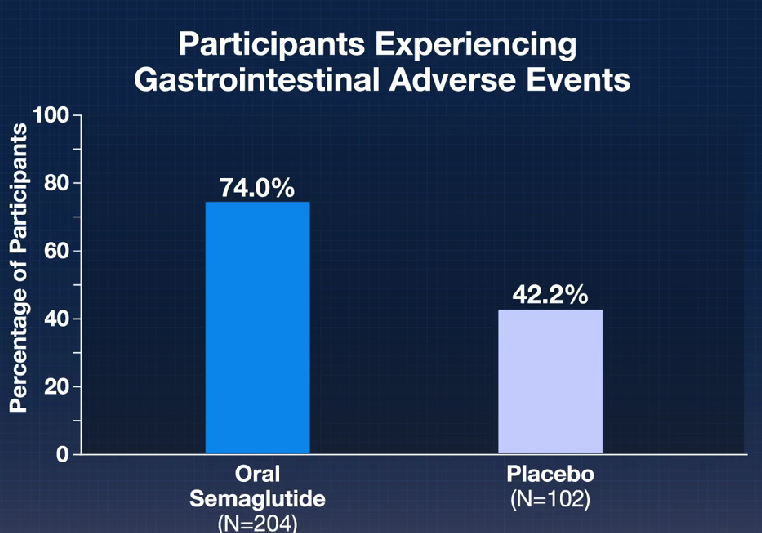
Methods: The participants were randomly assigned in a 2:1 ratio to receive oral semaglutide (25 mg) or placebo once daily, plus lifestyle interventions.
Key Findings:
In their discussion, the authors note that the reasons why “patients may prefer oral administration over the subcutaneous route are most often needle aversion and local skin reactions.7,8 In addition, unlike injectable agents, oral agents may not require a refrigerated chain of delivery and could widen the reach of obesity care in many regions of the world where a lack of refrigeration represents a barrier to access.”
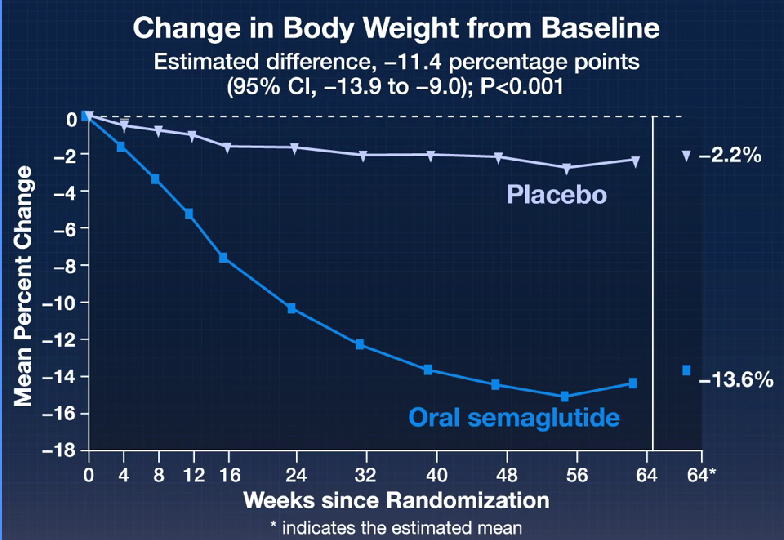
In addition, the results were similar to the “STEP 1 (Semaglutide Treatment Effect in People with Obesity) trial of weekly subcutaneous semaglutide at a dose of 2.4 mg (12.4 percentage points more than that with placebo),16“
As with prior trials of semaglutide, “treatment was also associated with substantial reductions in cardiometabolic risk factors including BMI, waist circumference, and levels of glycated hemoglobin, fasting plasma glucose, fasting serum insulin, lipids (very-low-density lipoprotein and triglycerides), and C-reactive protein.”
My take: Effective oral therapy is a big advance for management of obesity. The entire field of pharmacology for obesity has seen remarkable advances in the past few years. For me, it is reminiscent of the proliferation of published studies for hepatitis C around 10 years ago.
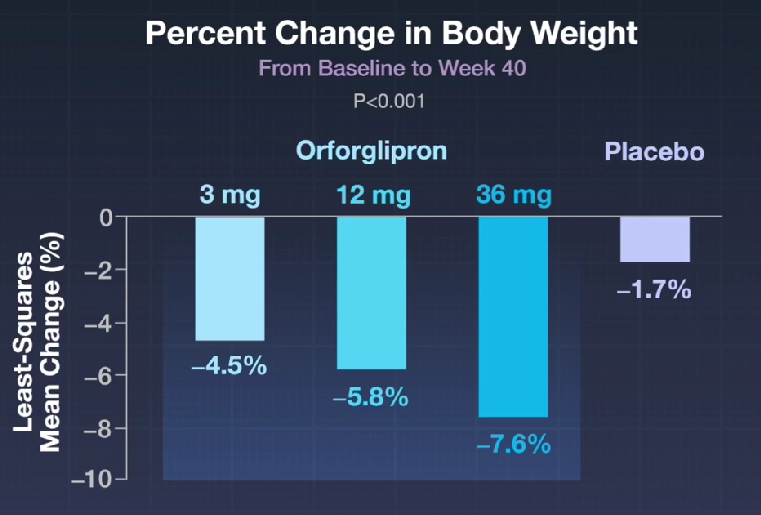
Related article in same NEJM issue: J Rosenstock et al. N Engl J Med 2025;393:1065-1076. Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist, in Early Type 2 Diabetes
In the ACHIEVE-1 Trial: Key Findings (n=559 adults):

The associated editorial by DB Lowe (N Engl J Med 2025;393:1133-1134) notes that Orforglipron is a small molecule that manages to mimic the effects of glucagon-like peptide-1 (GLP-1) at the GLP-1 receptor. “The incretins, like many peptide hormones, are fairly small as proteins go — a few dozen amino acids long. But that makes them gigantic as compared with small-molecule drugs. Their molecular weights are at least 10 times as high as the 300 to 500 mass units that medicinal chemists have traditionally aimed for, and being peptides, they have generally undesirable properties as well. Many have short half-lives in the circulation, which can be a desirable feature for endogenous peptides but is nowhere near what is needed for the administration of a once-daily dose.”
Related blog posts:
- Weight Loss Efficacy of Cagrilintide and Semaglutide
- “You Can’t Outrun a Bad Diet”
- FDA Approves Semaglutide for MASH
- Real-World Results of Obesity Pharmacotherapy With Tirzepatide and Semaglutide
- Head-to-Head: Tirzepatide Outperforms Semaglutide
- Impact of GLP-1 Agonists on IBD and Obesity
- Lifetime Health Effects and Cost-Effectiveness of Tirzepatide and Semaglutide in US Adults
- Semaglutide Keeps Weight Off at Four Year Mark
- Weight Gain If Semaglutide Stopped
- Jump in Knowledge Regarding Gut-Brain Axis
- GLP-1 Obesity Medication for 6-11 Year Olds
- Semaglutide in Adolescent Obesity
- Another Promising Medication (Retatrutide) for Obesity
- Oral GLP-1 Receptor Agonist for Obesity: Orforglipron (2023)
- Once-Weekly Mazdutide: Effective for Overweight and Obesity (GLORY-1 Study)
- Tirzepatide: Breakthrough in Obesity and Diabetes Management (SURMOUNT-1 Study at 3 years)
- Bariatric Surgery Declines as GLP-1 Medications Rise
- Survodutide, Dual Glucagon Receptor/GLP-1 Receptor Agonist, for MASH (Phase II Trial)
- Tirzepatide for Metabolic Dysfunction–Associated Steatohepatitis (MASH) & Uptick in GLP1 Use
