
E Stenke et al. Inflamm Bowel Dis 2025; 31: 2331-2337. Higher-Dose Infliximab Induction Achieves Better Maintenance Trough Levels in a National Pediatric IBD Cohort—A Retrospective Study
In this single center retrospective study from Ireland, the authors examined 122 patients (93 with Crohn’s disease [CD], 18 with ulcerative colitis [UC], 1 with IBDU) who received infliximab and had prospectively-collected data. The earlier cohort 2018-2019 received 5 mg/kg/dose and the later group 10 mg/kg/dose. Both groups had proactive therapeutic drug monitoring (pTDM).
Key findings:
- The 5 mg/kg group, compared to the 10 mg/kg group, was less likely to have target pre-third TLs (6% vs 80%, P < .001) with the stated goal of >/= 15 microgm/mL
- Fewer patients in the 5 mg/kg than 10 mg/kg group had pre-fourth TLs ≥5 µg/mL (6/48 [12.5%] vs 28/50 [56%], P < .001; mean [SD] TL 3.5 [6.3] vs 10.0 [9.9], P < .001)
- Concurrent immunomodulator therapy was more common in the 5 mg/kg group (43% compared to 24%)
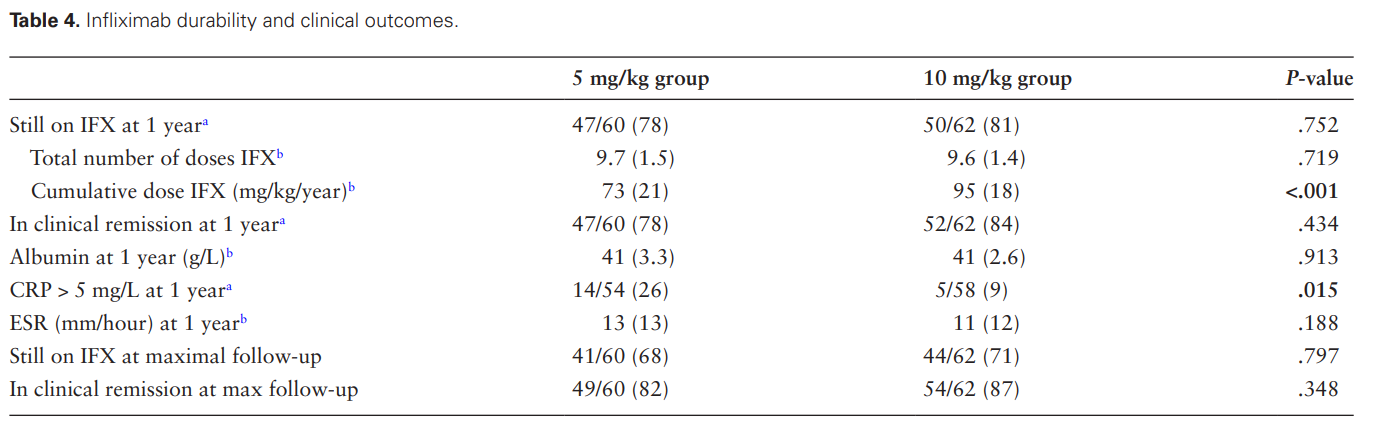
- 80% of patients were still receiving infliximab at 1 year including 87% of patients with CD and 54% with UC
- The higher dose group had a lower CRP at 1 year followup. 26% of patients receiving the lower dose had a CRP > 5 mg/L compared with 9% in the higher dose group.
- Some other measures of long term outcome (eg. IFX durability, clinical remission) were slightly better but did not reach statistical significance (see below)
Discussion Points:
- “Our data show higher rates of below-target infliximab levels during and after induction in the 5 mg/kg group. Higher rates of dose escalation in this group during the first year resulted
in similar dosing regimens…Thus, the similar infliximab durability and clinical outcomes
at 1-year follow-up reflect early-dose optimization leading to dose equalization between the 2 groups, rather than a lack of benefit to higher dosing regimens” - “Our data affirm that proactive TDM with pre-emptive dose escalation restores
below-target infliximab TLs and sustains clinical response…Indeed, in our cohort, some patients with low IFX levels pre-third dose were given their fourth dose 6 weeks later, rather
than the standard 8 weeks. Without proactive TDM results, our rate of suboptimal TLs pre-fourth and during maintenance therapy would have been higher in both groups” - “Rates of immunomodulator use in the 10 mg/kg group were lower than in the earlier cohort of 5 mg/kg, reflecting changes in clinical practice over time”
My take:
- This study shows that 94% of pediatric patients did NOT achieve adequate levels of infliximab at the pre-third dose with “standard” therapy. This was true even with 43% of the lower dose cohort receiving combination therapy (which often helps improve pharmacokinetics)
- Proactive therapeutic drug monitoring helped mitigate the clinical outcomes, especially in the lower dosed cohort
- “Children with IBD treated with the historic standard dose of 5 mg/kg induction are at increased risk of pharmacokinetic treatment failure related to high rates of suboptimal TLs”
Related blog posts:
- Infliximab: Reach Higher and Be Stronger
- Another Study Justifying Higher Infliximab Dosing in Pediatrics
- Proactive Therapeutic Drug Monitoring in Pediatric Crohn’s disease -Better Outcomes | gutsandgrowth
- Is Standard Infliximab Dose Too Low in Pediatrics?
- Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy for IBD? | gutsandgrowth
- Disease extent and need for higher infliximab dosing
- Proactive Therapeutic Drug Monitoring -Different Time Points | gutsandgrowth
- For the Next Insurance Appeal: Therapeutic Drug Monitoring in Adalimumab Treatment (Pediatrics) & Satire on Prior Authorizations | gutsandgrowth
- “Denials, Dilly-dallying and Despair”
- Kids Are Different: Therapeutic Drug Monitoring
- ARCH Study: Higher Doses of Infliximab in Acute Severe Ulcerative Colitis

Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
