
P Nicoletti et al. Gastroenterol 2023; 164: 454-466. Open Access! Identification of Reduced ERAP2 Expression and a Novel HLA Allele as Components of a Risk Score for Susceptibility to Liver Injury Due to Amoxicillin-Clavulanate
Key findings:
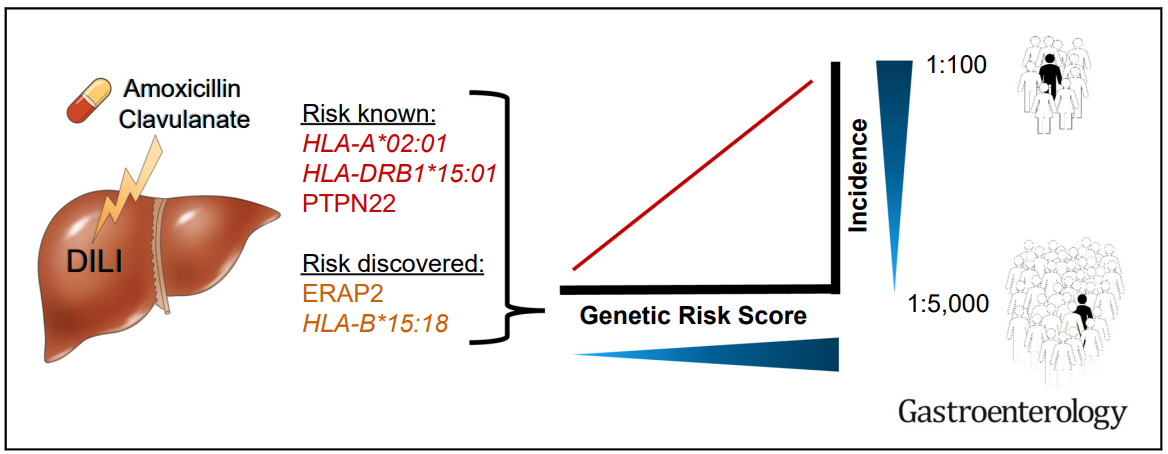
- Transcriptome-wide association study revealed a significant association of AC-DILI risk with reduced liver expression of ERAP2 (P = 3.7 × 10–7), coding for an aminopeptidase involved in antigen presentation
- “We also identified HLA-B∗15:18 as a novel AC-DILI risk factor in both discovery (OR, 4.19) and validation (OR, 7.78) cohorts”
- A genetic risk score incorporating rs1363907, rs2476601, HLA-B∗15:18, HLA-A∗02:01, and HLA-DRB1∗15:01, was highly predictive of AC-DILI risk when cases were analyzed against both general population and non–AC-DILI control cohorts.
- This genetic risk score does not apply to amoxicillin. “Clavulanate has long been considered the main component causing Amoxicillin-Clavulanate-DILI (LiverTox https://www.ncbi.nlm.nih.gov/books/NBK548517/).”
- While the genetic risk score has high specificity, it is not highly sensitive. “Our multimarker model based on the 5 risk alleles predicted approximately 13% of the total risk for AC-DILI, which is approximately one-third of the total DILI risk that has previously been attributed to common genetic variants (approximately 40%)”
My take: In cases of suspected AC-DILI, identifying an abnormal genetic risk could help confirm the diagnosis. However, due to low sensitivity it is not likely to gain widespread clinical use.
Graphical Abstract:
Related blog posts:
