Recently, Rachel Rosen gave a terrific review of reflux and reflux-related entities as part of our annual William (Billy) Meyers lectureship. This lecture information would be helpful for every pediatric gastroenterologist as well as every pediatrician, pediatric ENT, pediatric pulmonologist, pediatric SLP and lactation specialist. It puts to rest many obsolete ideas about reflux and its management. Some of her points have been covered by this blog previously (see links below) and by her bowel sounds podcast (see link below). Some errors of omission and transcription may have occurred as I took notes during this lecture.
Main points:
Reflux
- Using the label “GERD” increases the likelihood that an infant will be prescribed acid blockers; this phenomenon is noted as well with SLP and lactation specialist team members. Everyone needs to be careful about ascribing infant symptoms to “reflux disease”
- AR formulas need acid to increase their viscosity (don’t use PPIs in infants taking AR formulas). Also, AR formula viscosity is hindered when mixed with breastmilk (don’t mix with breastmilk)
- Most infants with reflux have nonacid reflux. PPIs do not help nonacid reflux
- PPIs are associated with increased aspiration and infection risks. Acid suppression has been associated with increased risk of allergic diseases
- Rumination can look a lot like reflux on pH probe studies
- Reflux hypersensitivity, and functional heartburn can result in similar symptoms as reflux (can be distinguished with pH testing)
- Pepsin can increase lung inflammation and can be increased by PPI use
- Red airway appearance is NOT indicative of reflux (poor specificity, poor sensitivity)
- If having symptoms with transpyloric feedings, this indicates that the symptoms are NOT due to reflux; transpyloritc feedings have similar efficacy as a fundoplication
- Avoid fundoplication. It does not result in fewer hospitalizations or improve pulmonary outcomes. It can result in a number of complications
- Consider genotyping for CYP2C19 pharmacogenetics in patients receiving chronic PPI. Those with rapid metabolism could benefit from higher doses. Those with slow metabolism could benefit from lower doses. Higher doses of PPIs increase risk for infections
- Bolus feedings result in fewer problems than continuous feedings
Delayed Gastric Emptying (Gastroparesis)
- Delayed GE is associated with increased lung bile acids. This is important in lung transplant recipients and increased lung bile acids is seen more commonly in those with frequent admissions for respiratory issues
- In Dr. Rosen’s experience, prucalopride is currently the most useful promotility agent in documented gastroparesis
BRUE:
- Infants with BRUE need to be tested for aspiration, not prescribed PPIs.
- VSS (aka OPMS) has the highest yield of any test in infants with BRUE (~72% abnormal testing in one study).
- Silent aspiration is common -don’t rely on SLP bedside assessment.
- Even with this diagnosis, many infants are still prescribed PPIs which increase the risk of complications (more hospitalizations, more infections, possible increase in allergies)
Aspiration:
- There are a number of potential etiologies, though most infants have aspiration due to neurological reasons (most transitory and improved by 7 months of age)
- In Boston, less than 5% with aspiration on VSS required GT placement
- Thickeners can be very helpful. Practitioners need to know the differences (don’t use Simply Thick in 1st year of life due to NEC risk)
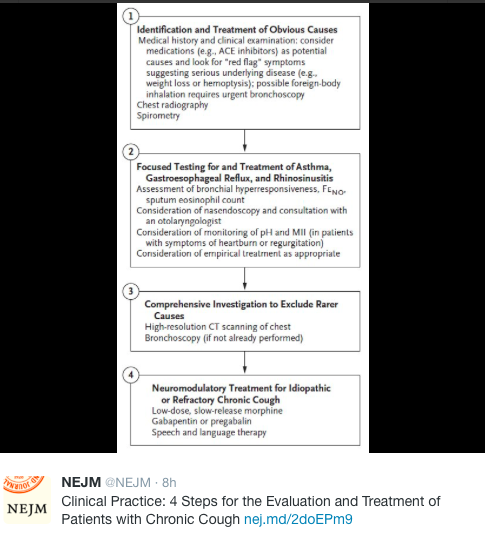
Chronic Cough:
- ~10% of kids with chronic cough have eosinophilic esophagitis (who have seen GI in Boston)
Related blog posts:
- Good Episode of Bowel Sounds on Reflux
- Acid Suppression for Laryngomalacia -Handed This Article to My ENT Colleagues
- Something Useful for Apparent Life-Threatening Events (ALTEs)
- Blaming Reflux for BRUEs -Not Changing Despite Guideline Recommendations
- Do Acid Blockers Given to Infants Increase the Risk of Allergic Disease?
- 2018 Pediatric Gastroesophageal Reflux Clinical Practice Guidelines
- Clinical evaluation not sensitive for aspiration
- How Many Kids with Reflux have Reflux?
- Better to do a coin toss than an ENT exam to determine reflux
- Hard Data on Blenderized Diets
- Treating reflux does not help asthma | gutsandgrowth
- How Likely is Reflux in Infants with “Reflux-like … – gutsandgrowth
- Which kids who aspirate need a gastrostomy tube?