A recent study (P Hopson et al. JPGN 2019; 68: 854-60) reports a high rate of isolated amylase deficiency of 10.1% in their cohort. Is this really accurate? I am skeptical.
- This is a retrospective study and the authors undertook endoscopic pancreatic function testing (ePFT) in a large number of patients, 712 over a 6 year period. The authors state “whenever there is clinical indication for esophagogastroduodenoscopy (EGD) we usually obtain” ePFT collections.
- To determine the amylase levels, the authors relied upon their in-house laboratory. Before accepting widespread deficiencies in amylase production, it would be useful to have specimens checked in more than one laboratory. At the same time, given the normalcy of the other pancreatic enzymes, it is likely that the specimens were of good quality.
- 59 of the 72 (82%) patients with isolated amylase deficiency were younger than 2 years. It is notable that in the same issue, some of the same authors in a review article describe the technique for ePFT (JPGN 2019; 68: 768-76) and note that amylase activity is undetectable at 1 month of age and is normal at 2 years of age. “Data are lacking as to when it is expected that most children have normal pancreatic amylase activity before 2 years of age.”
- The authors note that 48 patients (67%) with isolated amylase deficiency had failure to thrive or poor growth.
Amylase Levels:
- Looking at the authors’ Figure 1, they do provide their mean amylase levels; they considered a level below 10.3 micromol/min/mL to be deficient. Is this the right cutoff? Is there evidence that levels below this result in a disease state?
- Particularly in the first year of life, the amylase activities are much lower: approximately 2 micromol/min/mL for age 0-6 months and 12 micromol/min/mL for 6-12 months.
- In their cohort of 72 with abnormal amylase levels, 35 (approximately half) are less than 1 year of age. Thus, given how low the mean levels are, it is not surprising that nearly half of the patients (35/82) in this age group had abnormal ePFT.
- Even in the 1-1.5 year olds, the mean amylase activity is lower than the older group (approximately 24 micromol/min/mL compared to more than 40 micromol/min/mL for patients older than 6 years). The authors found 25% of the ePFT testing in this age group (1-15. yr olds) to have isolated amylase deficiency; again, this seems implausible.
- It is notable that there is not a control population. How often in healthy patients less than 2 years of age is the amylase level below their cutoff? In fact, the authors state that 10 of their patients with isolated amylase deficiency had constipation, and 5 had reflux which would be quite atypical presenting indications.
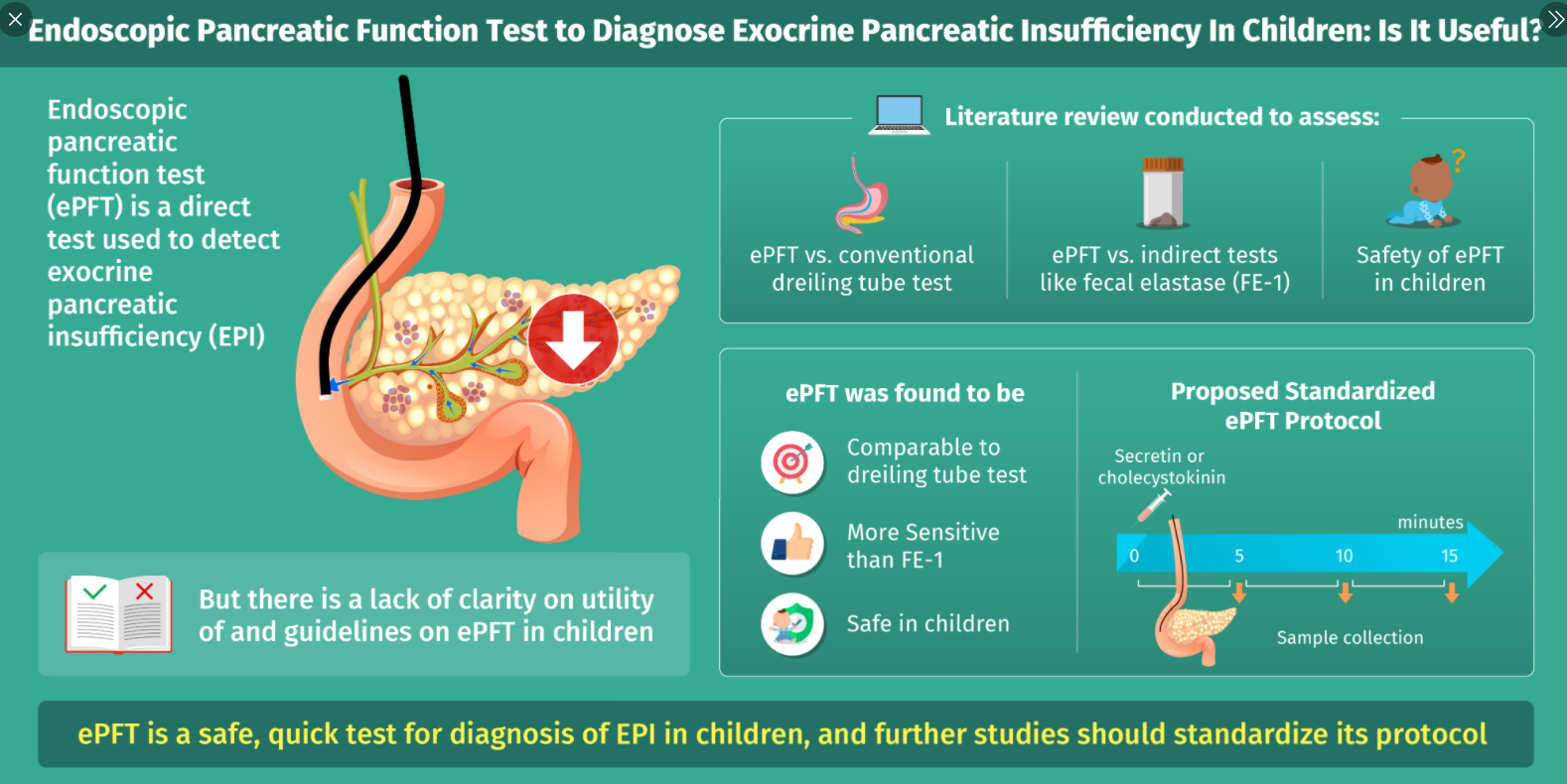
The technique for obtaining ePFT is detailed in the review (JPGN 2019; 68: 768-76) and includes the following:
- Before endoscopic intubation, “a bolus of secretin (0.2 mcg/kg to max of 16 mcg) is administered” (or alternatively synthetic CCK octapeptide in a dose of 0.02 or 0.04 mcg/kg).
- Initial fluid in stomach and duodenum is aspirated and discarded
- Using an aspiration catheter (or thru biopsy channel if scope too small), collect 3 to 4 aliquots of fluid between 3-10 minutes after injection of secretin (should be completed within 10 minutes of secretin)
- Place immediately on ice or dry ice
- Samples with low pH may be contaminated
- Avoid trauma to mucosa as bleeding can give erroneous results
I would suggest a more selective approach in utilizing endoscopy to check for both pancreatic function as well as disaccharidases. The sensitivity, specificity, positive predictive value and negative predictive value of a test is highly dependent on the study population. In those at low risk, the results of the testing is highly suspect.
My take: The reference to the review article is worth keeping as it gives a clear description of endoscopic pancreatic function testing. The study describing a 10% rate of amylase deficiency among a large cohort of pediatric patients requires careful interpretation, particularly as more than 80% of the deficiency group were less than 2 years of age. Clearly, a prospective study is needed. In those with possible isolated amylase deficiency at a young age (<2 years), a double-blind randomized trial may be needed to determine if enzyme supplementation is beneficial.
Related blog posts: Transient Exocrine Pancreatic Insufficiency or Misleading Tests?
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.