

Our Spooky Pumpkin
Here are some notes and a few slides from NASPGHAN’s plenary session. There could be errors of transcription in my notes.
Benjamin Gold, NASPGHAN president and part of our GI group, GI Care For Kids, welcomed everyone to the meeting.
Link to NASPGHAN_Annual_Meeting_Program 2019
Beth Carter Trophic Growth Factors: A Practical View
Key Points:
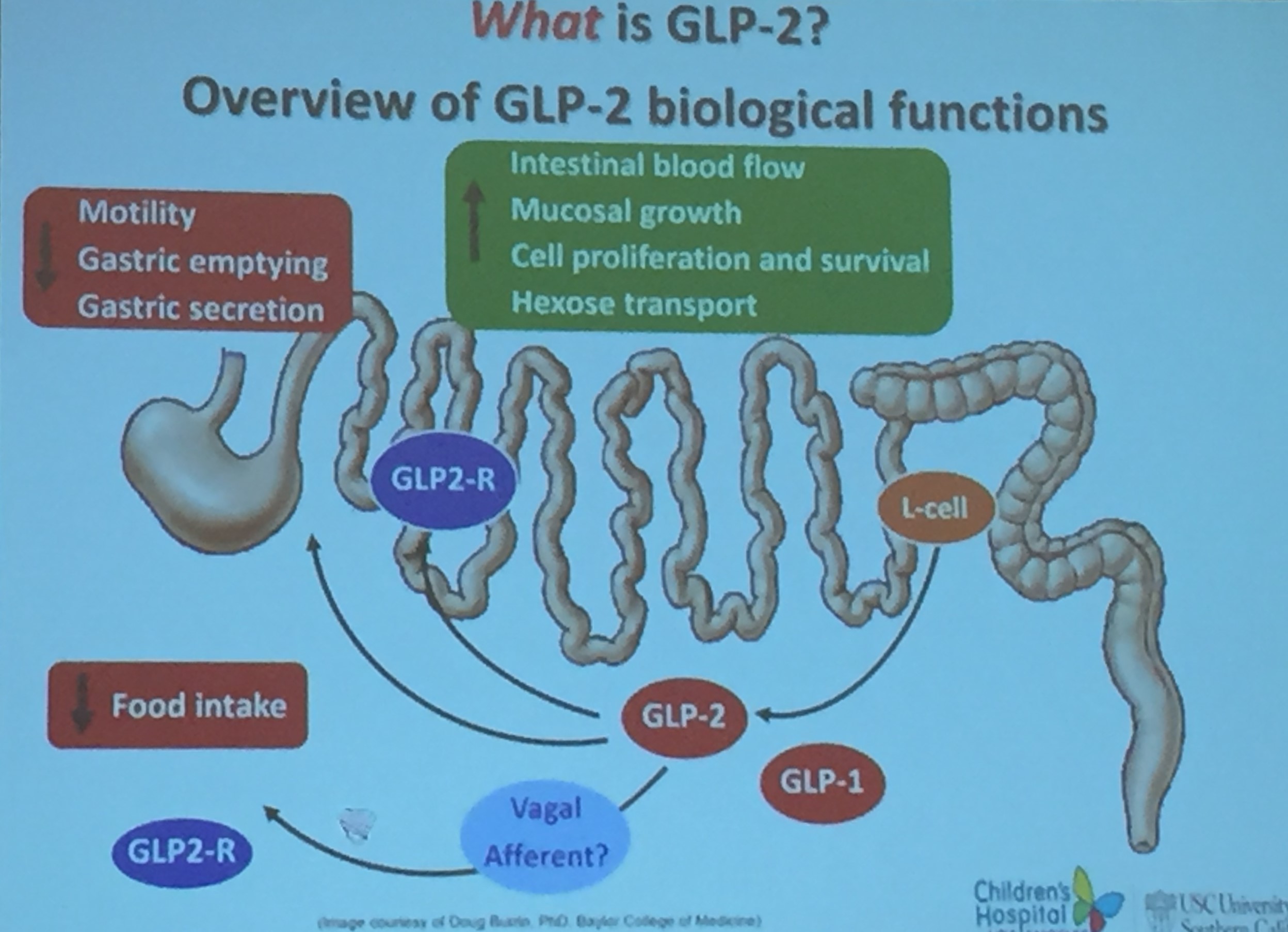
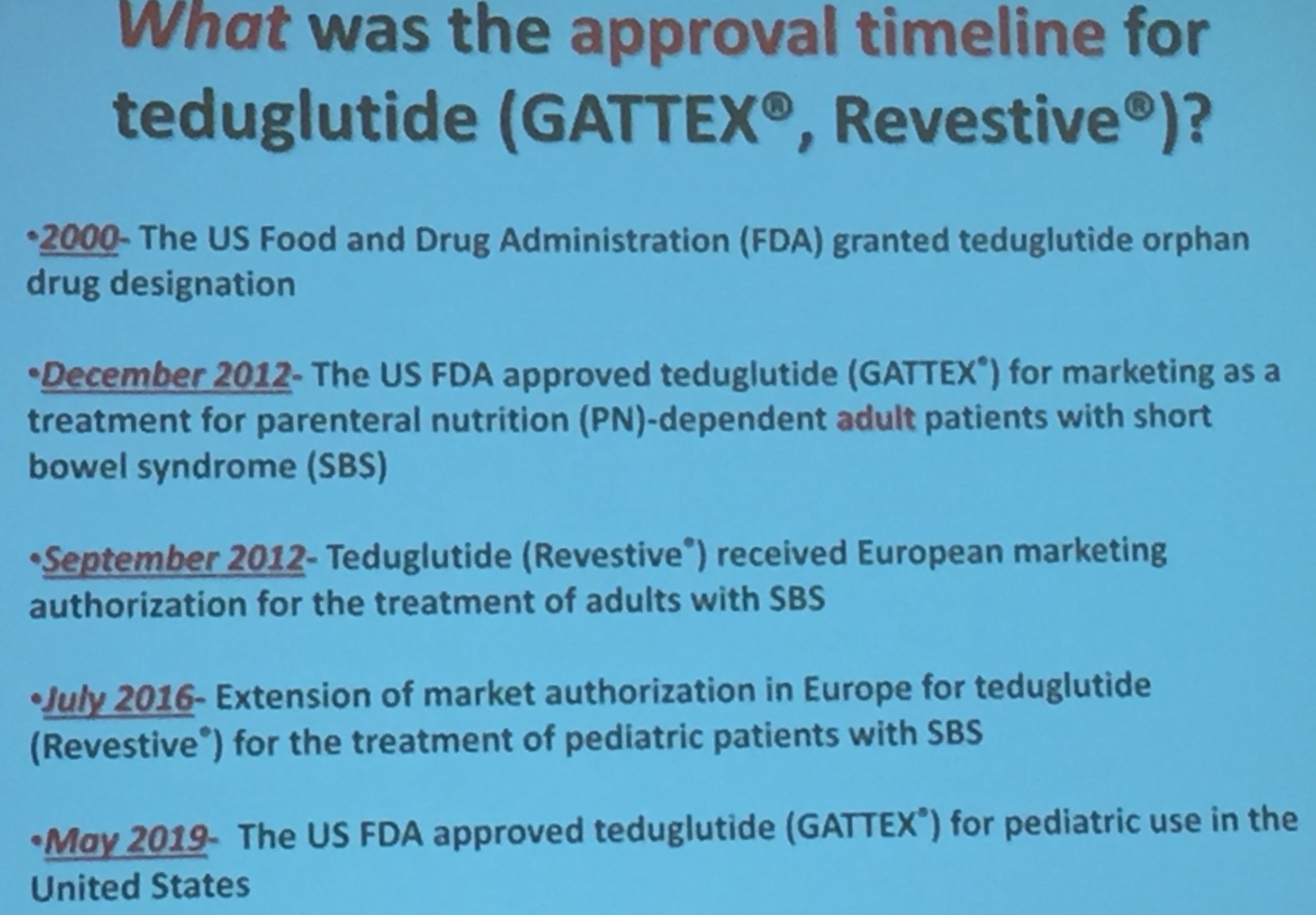
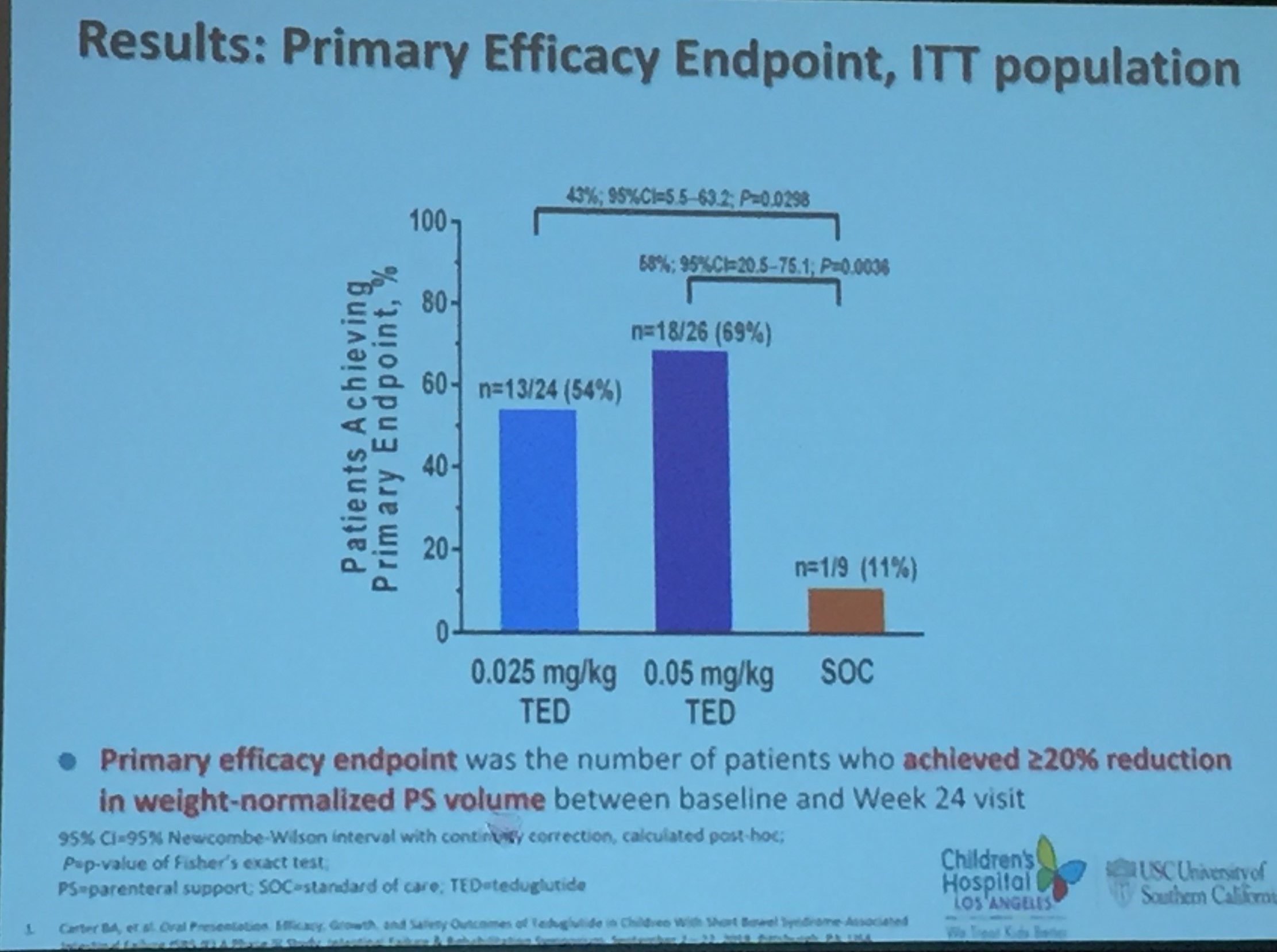
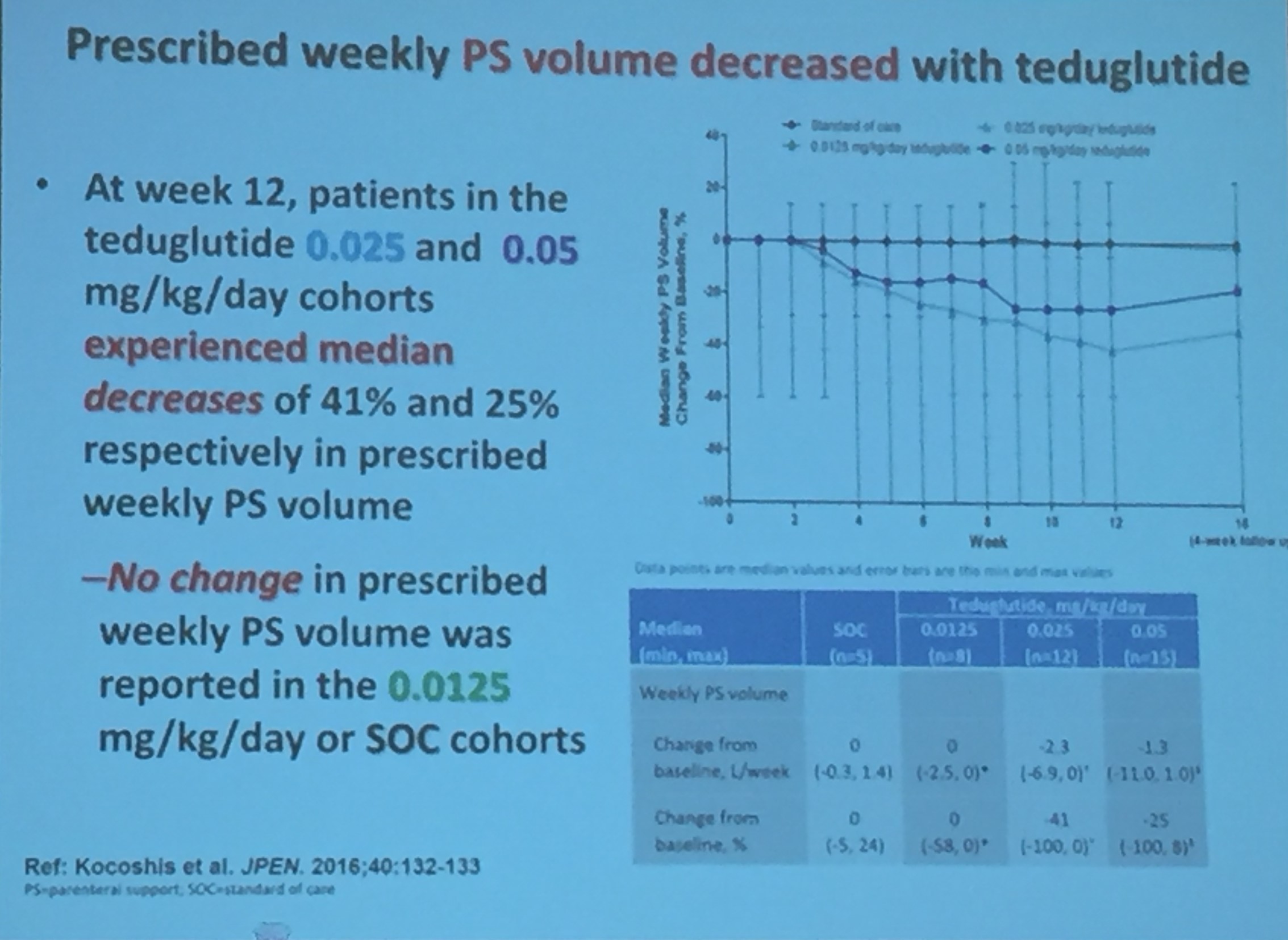
- GLP-2 has been approved as agent for intestinal failure for children (May 2019)
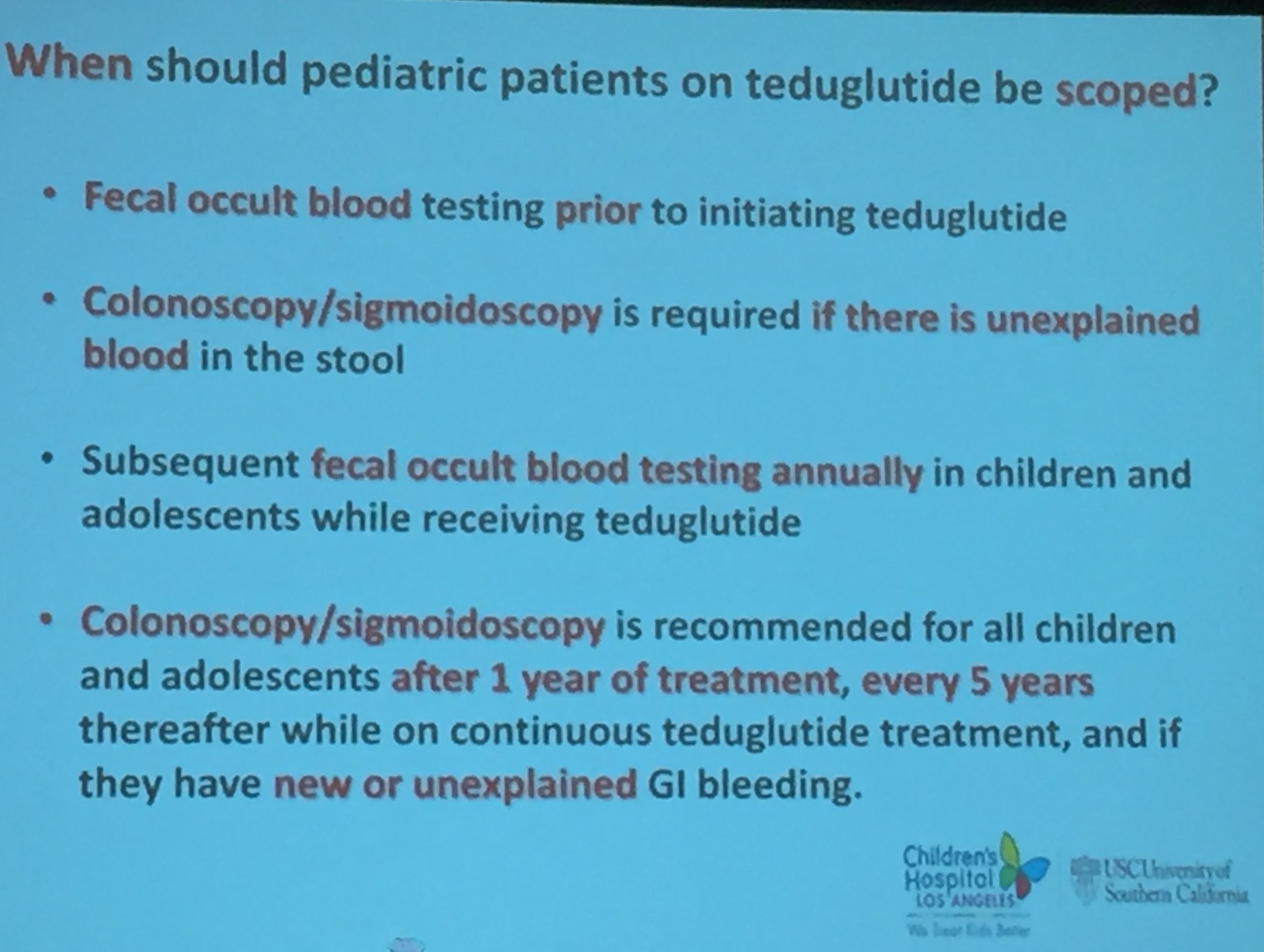
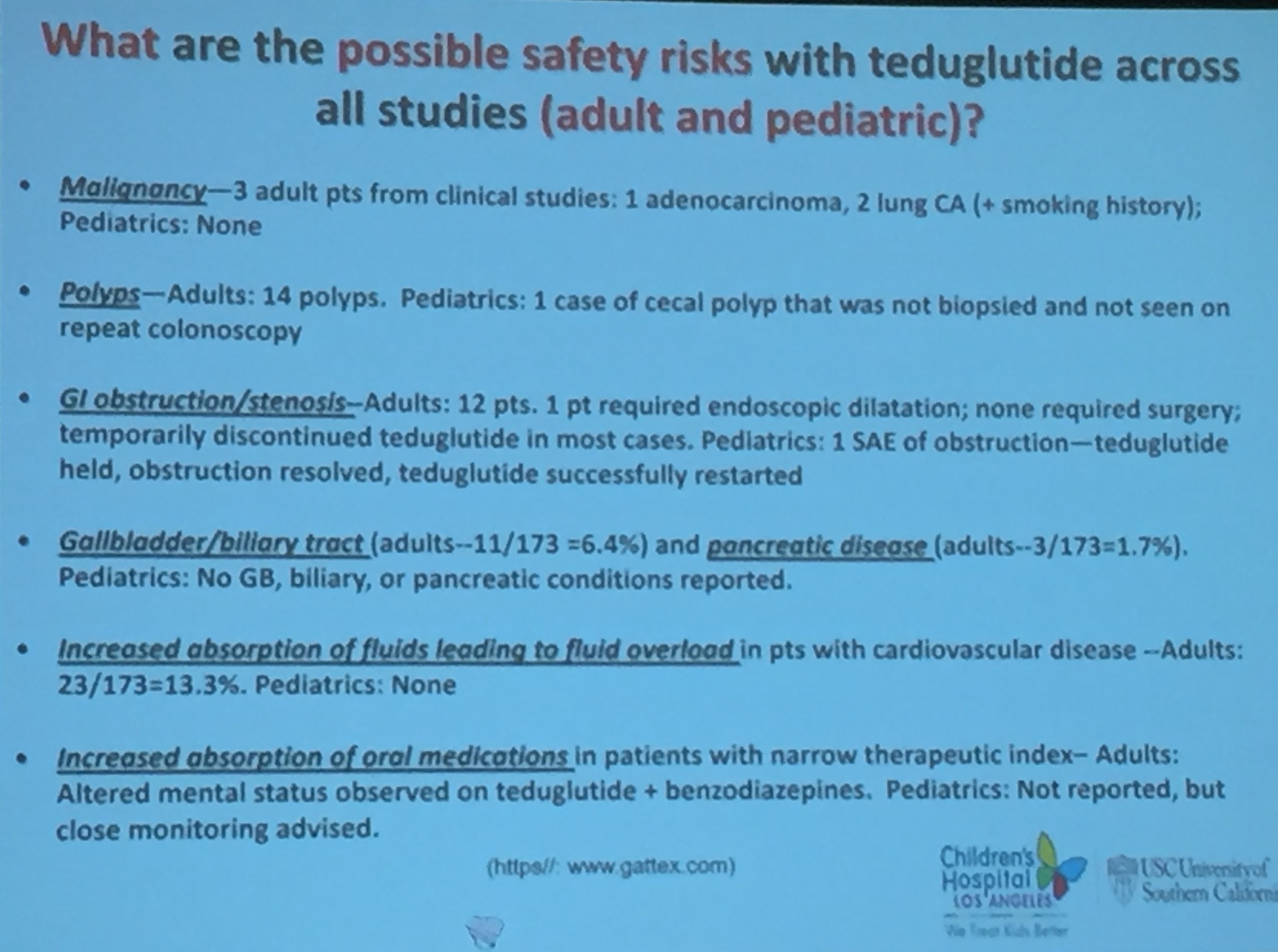
- Studies thus far have shown good safety but concerns remain (?increased risk of polyposis, increased growth of neoplasm) and as such increased surveillance needed for patients receiving GLP-2
- Cost in adults ~$295,000 per year
- Most patients need to continue GLP-2 to maintain effect








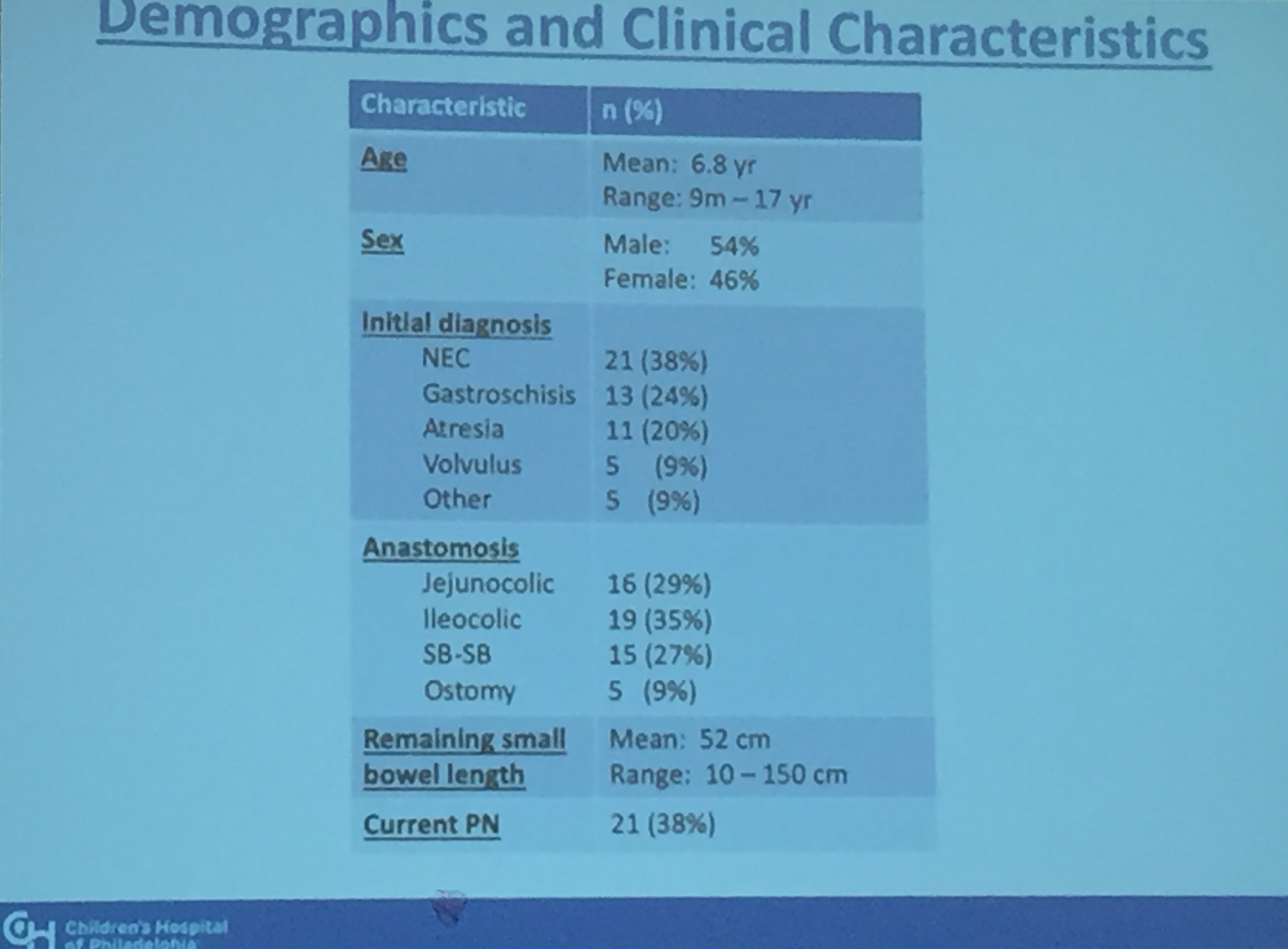
Arthur Kasti Abstract 218 Microbial Metabolites as Markers of Intestinal Dysbiosis in Pediatric Short Bowel Syndrome
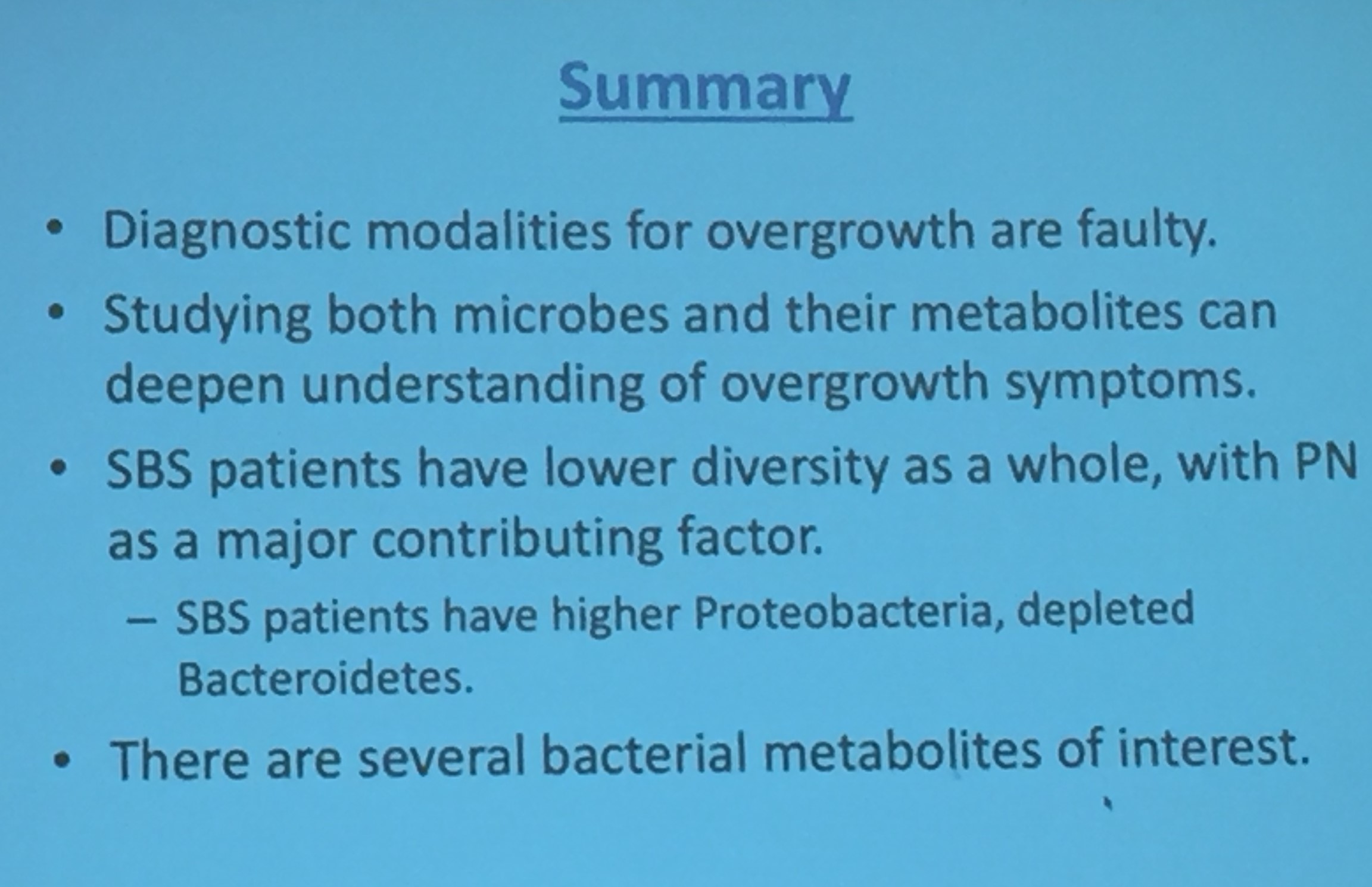
This was a terrific presentation. Key points:
- Microbiome in SBS patients is less diverse
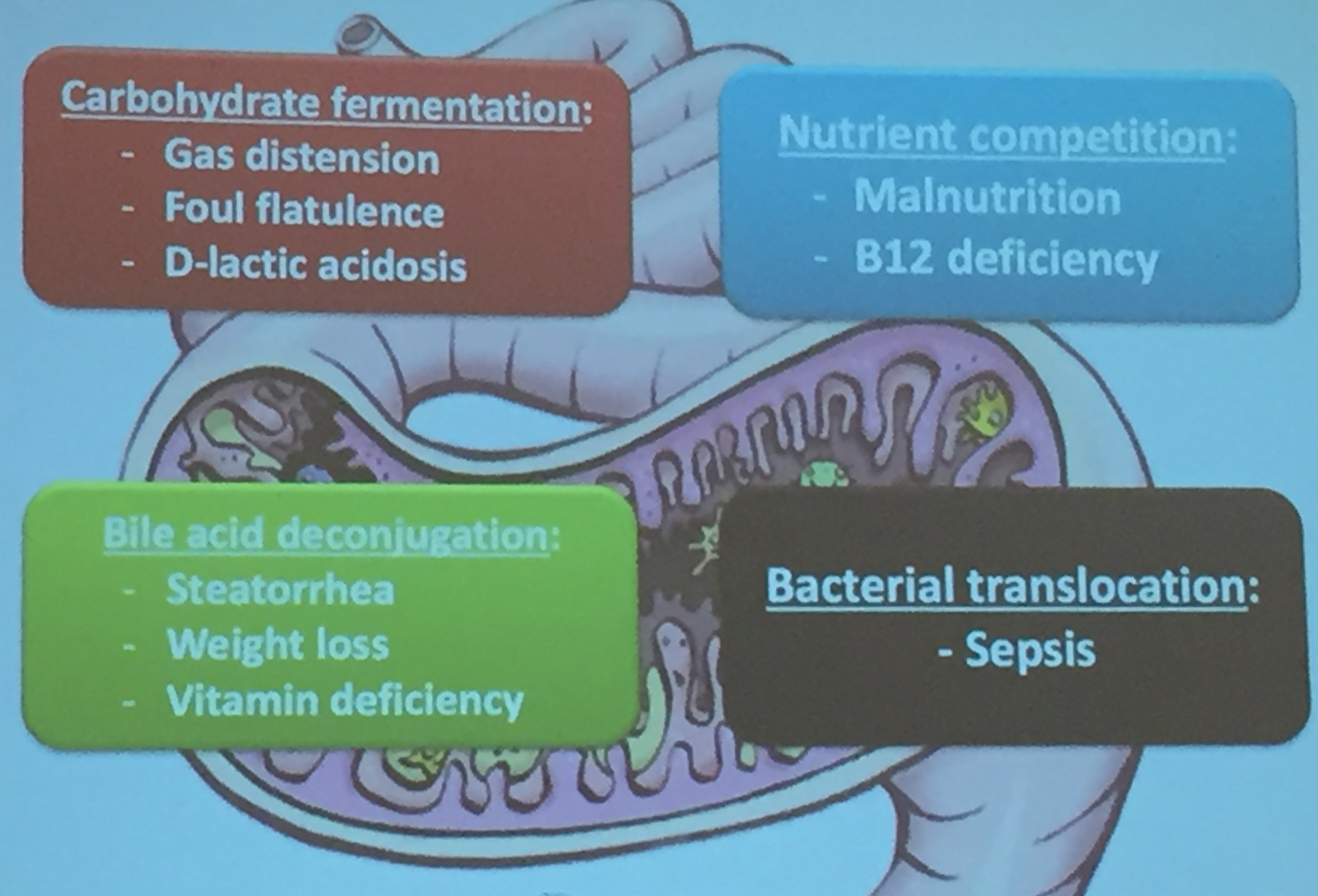
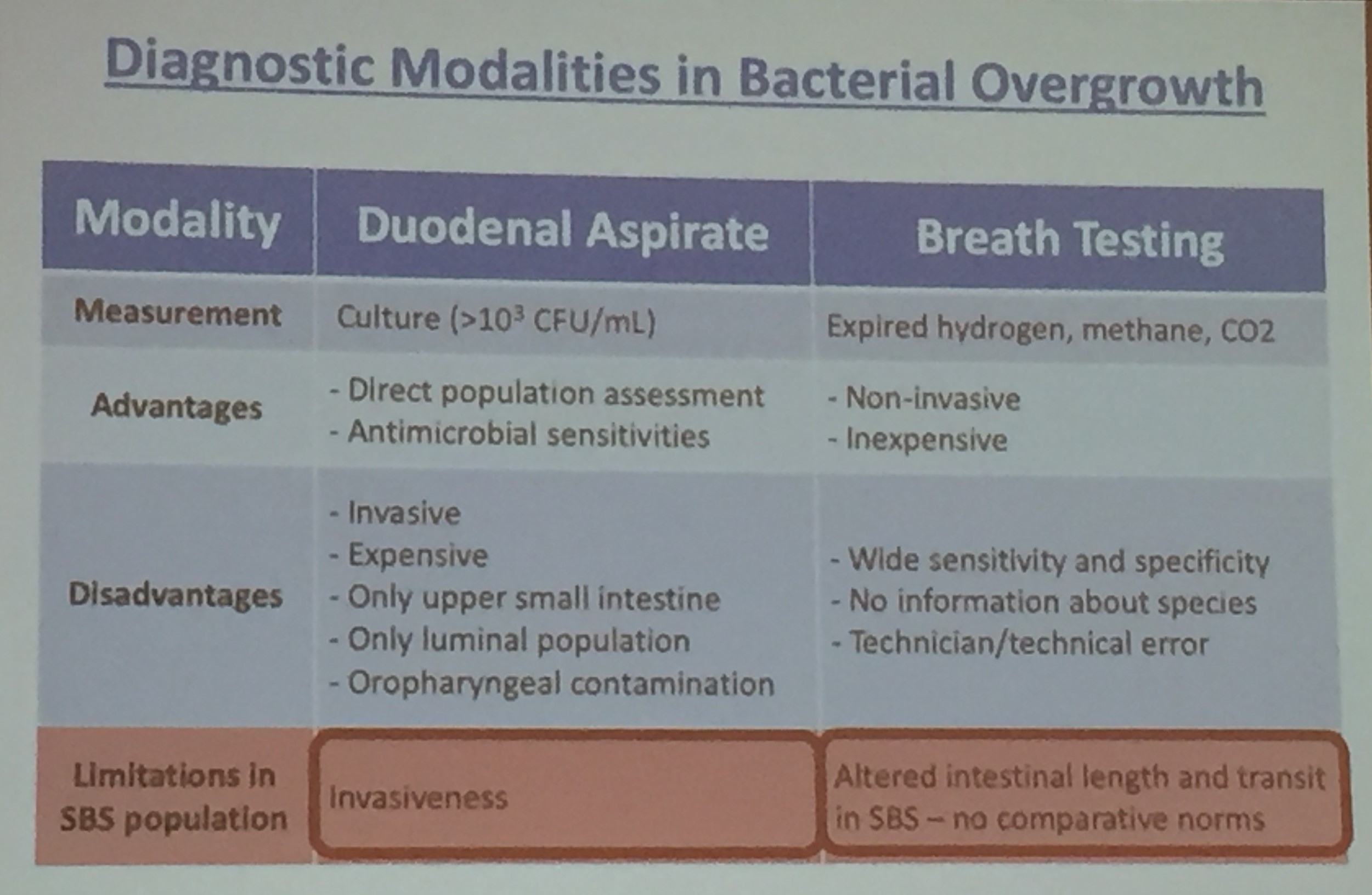
- Current diagnosis of bacterial overgrowth is difficult and definitive diagnosis is often impractical
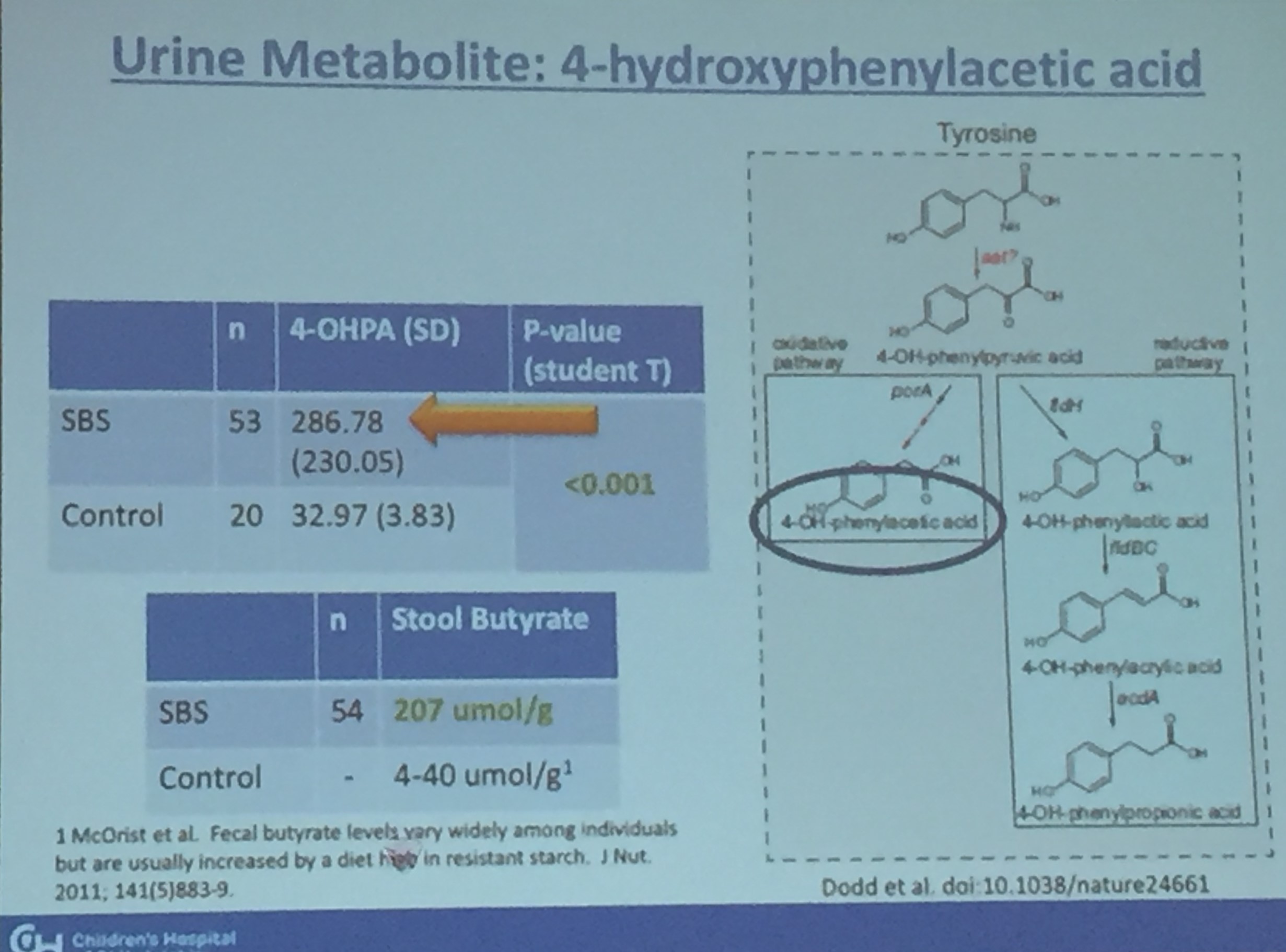
- Several metabolites may be helpful in diagnosis of bacterial overgrowth



Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
