From Vox: A CT scan costs $1,100 in the US — and $140 in Holland
An excerpt:
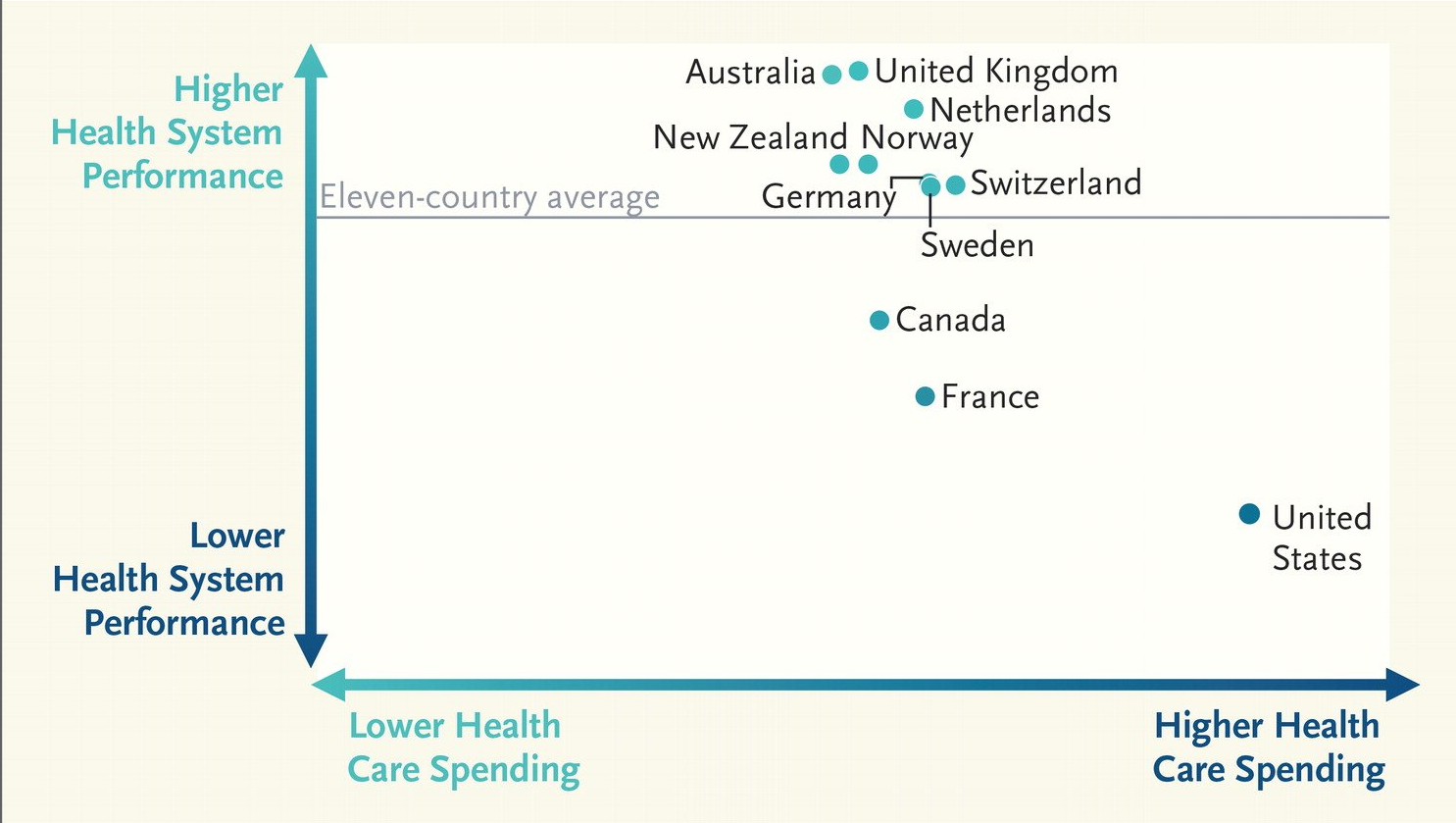
The Health Care Cost Institute put out a new report Tuesday showing how the prices paid for medical services by private insurance in the United States stack up against prices in other countries. As expected, American prices are collectively higher than the rest.
But four charts, based on the report, show just how thoroughly the United States is outspending other countries for almost every medical service or prescription drug.

Image Available on Twitter and Can be Found in Article

Related blog posts:
- Healthcare: “Where the Frauds Are Legal”
- Marketing of Insulin Explains a Lot About Our Health Care System
- Healthcare Costs Rising
- Do you know about the “Choosing Wisely… | gutsandgrowth
- Deriving Measures of High Value Pediatric Care | gutsandgrowth
- Value-based care | gutsandgrowth
- Implementing High-Value Care | gutsandgrowth
- What physicians can learn from fast-food restaurants… | gutsandgrowth
- 5000% Increase for Well-Established Drug | gutsandgrowth
- Some Hospitals Marking Up Treatments By As Much As 1000%
- Cornering the Generic Markup | gutsandgrowth
- Considering Cost in Treatment Choices | gutsandgrowth