PA Ubel et al. NEJM 2025; 392: 729-731. Out of Pocket Getting Out of Hand — Reducing the Financial Toxicity of Rapidly Approved Drugs
Key points:
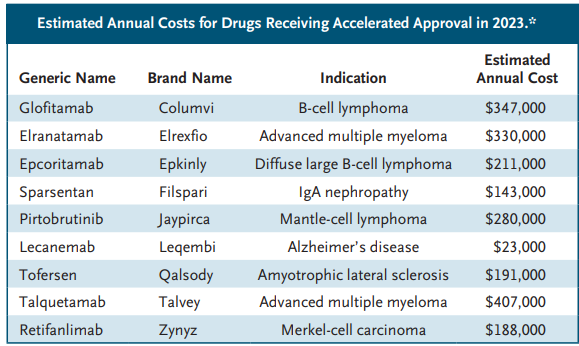
In 2023, the median list price of new drugs was $300,000 per year. The FDA does not consider drug cost as part of its approval process.
Many new drugs have uncertain benefits despite FDA approval. “Since the FDA is authorized to approve drug labeling, it could consistently require that labeling indicate when a drug’s approval was based on results from uncontrolled trials or from trials with surrogate measures…might reduce the chances that patients, seeing that a drug has FDA approval, will mistakenly assume that it has been proven to provide substantial benefits..[however] . In the face of serious illness, people frequently prefer action to inaction, even when they would ultimately be harmed by taking action.”
Optimally, “congress would need to pass legislation giving the agency authority to consider financial harms when making decisions about drugs with unclear benefits, and the FDA would need to gain expertise in evaluating the budgetary implications of new drugs.”
My take: The financial burdens of newer medications leave patients unable to afford other necessary medical and non-medical expenses. This is especially problematic when a new medication offers minimal benefit.
This article explains how generic and biosimilar companies have tried to navigate the ‘patent gamesmanship’ that brand-name manufacturers have used to delay competition for their products beyond the typical 20 years after an application is filed.
Key points from this article:
“The Hatch–Waxman Act, provided a partial solution by explicitly authorizing manufacturers to market generic drugs if they don’t claim any indications protected by active method-of-use patents.3 Such skinny labeling enables generics manufacturers to market their products for older, non–patent-protected indications without infringing later-issued method-of-use patents…43% of products that were the first available generic formulation of a brand-name drug included skinny labels”
The article delves into the GlaxoSmithKline v. Teva case which centers on the overlapping potential indications for the beta-blocker carvedilol. Teva had used skinny labeling to get approval for hypertension (HTN) but was sued by GlaxoSmithKline as carvedilol can be used for congestive heart failure (CHF).
Much of the case centers on the paradox that “by law, generics [& biosimilars] manufacturers are required to use very similar labels” as the labeling of original products even though the generic has requested approval for a much narrower approval. In this case, when the Teva generic was used for CHF, GlaxoSmithKline sued since the product was approved for HTN.
Another example: Humira has “more than 70 patents on inventions ranging from the active pharmaceutical ingredient and primary indications to the drug’s purity, various formulations, and secondary indications.” For a generic/biosimilar to address all of these (potentially-endless) patents is a huge barrier.
Based on this ruling, “brand-name manufacturers can thus now create labels that reference material related to new method-of-use patents and then sue generics manufacturers for patent infringement.”
“Lack of action by both the Supreme Court and Congress would allow brand-name drug manufacturers to wield a powerful new weapon to delay or deter the entry of generic and biosimilar drugs, which could have important implications for health care costs and patient welfare.”
My take: My prediction is that these tactics by drug manufacturers, despite their extensive financial connections with lawmakers, will eventually backfire and result in extensive changes to the regulations regarding exclusivity and pricing.
In an unrelated article in the same issue, Golda Grinberg provides a first-hand account of how families could benefit by the consideration of hospice in children with extensive medical problems. NEJM 2023; 388: 486-487. Please Look at My Baby — When Clinicians Should Say the Word “Hospice”
“To the surprise, perhaps even shock, of the SICU team, we tossed an option B onto the table: if we truly could not extubate, we suggested, maybe we should skip the trach and transition to comfort care….When presented with a child in whom previous extubation attempts had failed and who was becoming more deconditioned by the day, the SICU team had made the standard, safe, and familiar recommendation for an acute problem: place a trach… It would have been tremendously helpful if, from the beginning, we’d had an open conversation with our son’s medical team and discussed all the options.”
My take: Most parents are happy with their medical decisions for their children. However, it is not uncommon to hear parents say many years later that they wished that they had been informed of the long-term dire outlook of their children and the possibility of deescalation of care in children with severe medical conditions before embarking down the ‘standard’ path.
This article details how AbbVie has perfected the use of patent protections to extend its monopoly over adalimumab; this has been to the detriment of many patients , employers and taxpayers who bear the additional costs. Key points:
In 2016, a blockbuster drug called Humira was poised to become a lot less valuable. The key patent on the best-selling anti-inflammatory medication, used to treat conditions like arthritis, was expiring at the end of the year…Through its savvy but legal exploitation of the U.S. patent system, Humira’s manufacturer, AbbVie, blocked competitors from entering the market.
Since the end of 2016, the drug’s list price has gone up 60 percent to over $80,000 a year, according to SSR Health, a research firm.
Patents are good for 20 years after an application is filed. Because they protect patent holders’ right to profit off their inventions, they are supposed to incentivize the expensive risk-taking that sometimes yields breakthrough innovations. But drug companies have turned patents into weapons to thwart competition. AbbVie and its affiliates have applied for 311 patents, of which 165 have been granted, related to Humira, according to the Initiative for Medicines, Access and Knowledge, which tracks drug patents. A vast majority were filed after Humira was on the market.
The article notes that one employer has been flying a patient receiving Humira to the Bahamas to pick up her medication.
AbbVie … will have a new way to make more money from the drug. Under the terms of the legal settlements… AbbVie will earn royalties from the knockoff products that it delayed.
In the longer run, though, AbbVie’s success with Humira may boomerang on the drug industry. Last year, the company’s tactics became a rallying cry for federal lawmakers as they successfully pushed for Medicare to have greater control over the price of widely used drugs that, like Humira, have been on the market for many years but still lack competition.
My take: It makes me mad when I read this article. First of all, there are a lot of patients harmed by this gaming. Second, it is outrageous that the cost of this expensive medication was raised 60% over the last 6 years (and going up 8% more in 2023). Third, I am disappointed to learn that AbbVie will still make money off biosimilars because I am looking forward to NOT using Humira because of these tactics. Lastly, I hope that this does prompt legislative/regulatory changes to limit this practice going forward.
Drugmakers are able to extend the patents on their drugs, keeping generics off the market, through a process known as “evergreening”… The excessive use of the patent system — by drugmakers Bristol-Myers Squibb, AbbVie, Regeneron and Bayer — keeps the prices of the medications at exorbitant levels, often at the expense of American consumers, according to the report from the Initiative for Medicines, Access & Knowledge, or I-MAK, a nonprofit organization that advocates drug patent reform.
“They get the power, they get the monopoly and they start hiking their prices,” said Priti Krishtel, a health justice lawyer and a co-founder of I-MAK…
The U.S. patent system is meant to reward innovation by permitting drug companies to sell new medications on the market and barring other manufacturers from making generic versions for a set period of time — usually 20 years. Once the patent expires, generics are allowed on the market, often at a lower list price than the brand-name drug.
But drugmakers often extend their patents by making small tweaks to the drugs, sustaining their monopolies for several years...
Humira, a rheumatoid arthritis drug from the Chicago-based biotech firm AbbVie, generated $17.3 billion in annual sales in 2021. There are 311 patent applications for the drug, 94% of which were sought after FDA approval. AbbVie’s original patent on the drug expired in 2016, but it won’t face competition until 2023...
The practice of extending patents doesn’t always go unchallenged. In some cases, generic manufacturers sue the drugmakers to get their drugs on the market, Lemley said. However, he added, those lawsuits often end in settlements between the companies.
My take: As bioethicist Arthur Caplan states, this is an unethical practice and “we need to be rethinking the rules of patenting.” There is no good reason why patients in the U.S. need to be paying 5 times as much for adalimumab as patients in Europe.
During the pandemic, several of the pharmaceutical companies have helped improve the reputation of the industry by expeditiously developing life-saving therapies and vaccines. At the same time, many have continued with outrageous price increases of generic medications. An example of this is rectal indomethacin which is used for the prevention of pancreatitis after ERCP. In this commentary, the key points:
The current price in the U.S. for this previously inexpensive medication is now $429 (in 2021) (previously $17). For patients, this charge is often multiplied by hospital billing departments and is frequently NOT covered by insurance as the manufacturer has not filed a new drug application with the FDA (new indication).
The authors note that rectal diclofenac would be a suitable alternative with similar (?better) effectiveness but is currently not available in U.S.
The government could allow importation of either diclofenac or indomethacin (see Table below for costs of these medications in other countries). “If the government used the powers granted in the Medicare Modernization Act of 2003, the price gouging problem caused by rectal NSAIDs could be swiftly solved without the need for expanding the US manufacturing market.” This would drop the “price of this potentially lifesaving prophylaxis by 99.24%.”
My take: I am still grateful to Mark Cuban (Why I No Longer Need to Be A Billionaire | gutsandgrowth) who is much more likely to fix the generic drug pricing problem than our government which has been reluctant to take measures against big pharma.
This commentary notes that the National Institutes of Health (NIH) spends more than $40 billion each year to fund biomedical research. “We believe that medicines discovered at public expense should be affordable.”
A Few Excerpts:
“Existing laws provide two paths for achieving this result. First, the Bayh–Dole Act of 1980 gives the government a royalty-free license to use patented inventions that were discovered using federal funding. The government has never exercised its Bayh–Dole license”
“Second, 28 U.S. Code §1498, which dates to 1910, gives the government immunity from being sued for patent infringement in federal courts, while giving patent owners the right to receive reasonable compensation when the government makes or uses a patent-protected product”
Case in point: “Recently, the government signed a contract with Merck to purchase molnupiravir (Lagevrio), an oral antiviral drug that reduces the severity of Covid-19. The contract price of $712 per treatment is estimated to be more than 35 times the cost of producing the drug at a reasonable profit. Molnupiravir was discovered at Emory University using government funding, and Emory’s patent applications acknowledge the government’s Bayh–Dole license.5 Molnupiravir payments for Medicare, Medicaid, and VHA patients could cost the government billions in 2022. This amount could be reduced by more than 90% if the government exercised its license and allowed a generic manufacturer to supply the drug for patients in government-supported programs.”
My take: U.S. taxpayers should get a return on their investment when new medications are developed with government funding rather than paying more for these medications than any other country.
Fortune Dec 2021-Jan 2022: Insulin’s Deadly Cost Thanks to Stan Cohen for sharing article.
Some excerpts/key points:
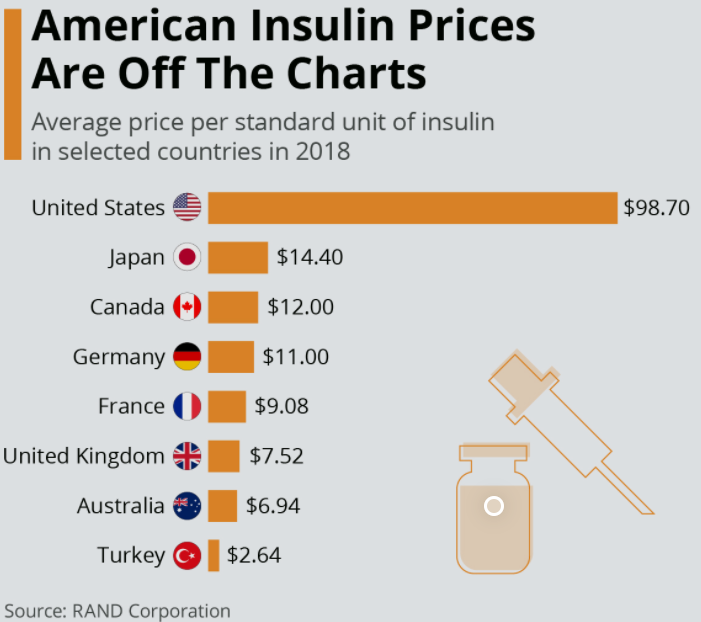
“Insulin in the U.S. costs on average some 800% more than in other developed economies. And yes, people die for lack of it, sometimes within days or even hours of missing their dose. No one knows how many; data suggests that in the U.S. it’s at least a few every day. Far more may suffer other ravages of diabetes—blindness, heart attacks, loss of limbs.” In addition, 40% of Americans who have died from COVID-19 were diabetics.
“Manufacturer’s compete not by cutting prices but by raising them.” This is often due to pharmacy benefit managers (PBMs), the middleman between manufacturer’s and insurers. PBMs negotiate drug prices and establish formularies. PBMs make more money if they able to discount higher rebates on the list cost; hence, to influence PBMs to choose their products, manufacturer’s are incentivized to raise drug costs, even if the average price is unchanged. Higher list prices affect those least able to cover the costs, namely those without insurance as well as many with high deductibles.
List price for Humalog (Eli Lilly) more than doubled from 2013 to 2018, Lantus (Sanofi) more than quadrupled from 2005 to 2016
Some patients have obtained insulin in Canada where costs for a vial could be more than 10-fold less (though this is illegal). There are also more than 12,000 GoFundMe.com listings with “insulin” in the title.
For the insulin market, some recent changes include the emergence of GLP-1 analogs for Type 2 diabetes (~90% of diabetes in U.S.). Trulicity is now Eli Lilly’s bestselling medication. In addition, the FDA recently approved Semglee, an interchangeable biosimilar for Lantus which is reducing costs.
My take: “The story of insulin is a poster child for everything that’s wrong with a free-market approach to drug availability,” says Arthur Caplan…”It’s almost inexcusable morally.”
The one common feature is that these are all very expensive; there are many other expensive medications with less benefit. Given the rise in costs of these medications, there is a need to do a better job in getting good value in our drug costs. A potential path forward is outlined in a recent commentaries (SB Dusetzina, J Oberlander. NEJM 2019; 381: 2081-4; PB Bach. NEJM 2019; 381: 2084-6).
In the first commentary, the authors review the Elijah E Cummings Lower Drug Costs Now Act of 2019 (HR 3).
In essence, this act establishes a drug-price negotiation process and limits price increases on existing products. “Companies whose products are selected for ‘negotiation’ will in reality face price regulation and a severe penalty for noncompliance.”
The act would examine U.S. prices compared to prices paid in other countries. “There would also be a legislatively set maximum price that could not exceed 120% of the average net price paid for the same drug in designated countries.”
The bill also would cap Medicare Part D out-of-pocket spending at $2000 per year.
In the second commentary, Dr. Bach notes that drugs that have too little evidence to support full approval and those that are ‘too late in their life cycle’ both should have their pricing negotiated by the government. This would side step some of the arguments about undermining the incentive for new drug development.
“Too little”
The FDA grants approval of some drugs on the market conditionally on the basis of data indicating that they improve a surrogate marker of patient benefit. “Despite the conditional nature of the approval, …the pharmaceutical firms currently charge the same high prices that fully approved drugs capture.”
Required studies frequently show that these conditionally-approved medications are ineffective. Of the 198 indications granted accelerated approval since 1992, only 115 have garnered full approval. Also, conditional approval may result in less incentive to complete the needed trials in a timely fashion.
“Too late”
In this category, the author notes that some medications have found many ways to extend their monopolies, which are intended as a time-limited reward for the effort of developing a new medication. These include overlapping patents, refusing to provide samples to competitors, and paying other companies to delay bringing generic or biosimilar products to market
Most of the potential for savings are in this category rather than the ‘too little’ category
Negotiating prices of the top 10 too little and 10 too late medications with reference to 120% of UK pricing would have provided about nearly 27 billion in savings in 2019
My take: While current partisanship makes reaching agreement difficult, targeting soaring pharmaceutical costs is one area in which I predict common ground can be found. While many are going to benefit from the therapeutic advances listed above, there are other medications which are overpriced and should be negotiated like in other high-income countries.
A recent commentary (M Fralick, AS Kesselheim. NEJM 2019; 381: 1793-5) describes the U.S. Insulin Crisis.
Background:
In 1922, insulin was first injected into a 14-year-old boy with severe type 1 diabetes mellitus (T1DM). Prior to this, T1DM had been considered a universally fatal disease
Frederick Banting, John Macleod, and members or their team that discovered insulin sold their patent for $1 to assure it could be widely affordable
“U.S. law allows pharmaceutical manufacturers to price their products at whatever level they believe the market will bear and to raise prices over time without limit”
“Direct competition in the insulin market is lacking”
Since insulin is a biologic drug, this necessitates “additional testing beyond what is usually required for generic drugs before approval by the” FDA.
Current Situation:
A carton of insulin that sells for $300 in the U.S. could be purchased in Canada for $20 (in U.S. dollars)
Nearly 100 years after the development of insulin, “insulin is inaccessible to thousands of Americans because of its high cost.”
My take: Why does insulin cost 15 times more in the U.S. than Canada? These excess costs with insulin are occurring despite a great deal scrutiny; unfortunately, U.S. consumers are paying extra for a wide range of pharmaceuticals. Going from the Nobel discovery of insulin to our current state is a clear indication of the need to reform of our healthcare system.
The average cost of a brand-name drug was 18.6 times higher than its generic equivalent in 2017, and the size of that gap has more than tripled since 2013, according to a report from the AARP Public Policy Institute…
In 2017, the average retail cost of 260 generic drugs widely used by older adults for chronic conditions was $365 for a year of therapy, compared with $6,798 for brand-name drugs. In 2013, that same year of therapy with an average brand-name drug ($4,308) was only 5.7 times more expensive than the generic ($751)…
“Generics account for nearly 9 out of every 10 prescriptions filled in the U.S. but represent less than a quarter of the country’s drug spending,” Debra Whitman, executive vice president and chief public policy officer at AARP
My take (borrowed in part from Debra Whitman):
“These results highlight the importance of eliminating anticompetitive behavior by brand-name drug companies so that we get more lower-priced generic drugs on the market”
This data shows the alarming increase in cost of brand-name medications.