WSJ: How Pfizer Set the Cost of Its New Drug at $9,850 a Month
An excerpt:
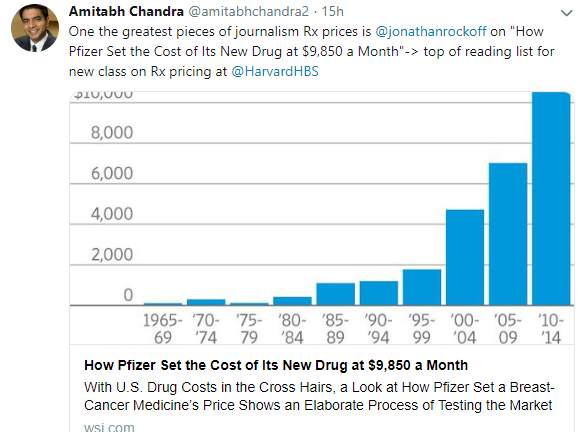
The average cost of a branded cancer drug in the U.S. is around $10,000 a month, double the level a decade ago
Pfizer’s multistep pricing process shows drugmakers don’t just pick a lofty figure out of the air. At the same time, its process yielded a price that bore little relation to the drug industry’s oft-cited justification for its prices, the cost of research and development.
Instead, the price that emerged was largely based on a complex analysis of the need for a new drug with this one’s particular set of benefits and risks, potential competing drugs, the sentiments of cancer doctors and a shrewd assessment of how health plans were likely to treat the product…
In 2013, Pfizer hired outside firms to conduct hourlong interviews with more than 125 cancer doctors in six cities…
Pfizer hired firms that surveyed more than 80 health-plan officials such as medical directors and pharmacists…
Pfizer employees say the mock reviews supported a monthly price below $10,000. If it was higher, insurers could start requiring doctors to fill out paperwork justifying its use.
My take: This article makes clear that the driver of higher pharmaceutical prices is based on a shrewd assessment of what the market will bear.
Related blog posts:
- Upside Down Incentives in Pharmaceutical Development –Profit over Patients
- 5000% Increase for Well-Established Drug | gutsandgrowth
- Drug Waste Costing Billions. Who benefits? Pharmaceutical Companies
- Public Shaming is Not an Effective Drug Pricing Policy | gutsandgrowth
- How to Undermine Value Care: Lessons from Pharmaceuticals | gutsandgrowth
- Orphan Drugs –Very Profitable | gutsandgrowth
- Turning Liquid into Gold: A Pharmaceutical Rumpelstiltskin Story | gutsandgrowth
- Another Shady Pharmaceutical Business Practice: Citizen’s Pathway to Delay Competition | gutsandgrowth
- Does it really cost $2.6 billion to bring a new drug… | gutsandgrowth
- This Is A Stick Up — Your Money or Your Life” | gutsandgrowth
- Buyer Beware: Supplement at Your Own Risk | gutsandgrowth
- Cornering the Generic Markup | gutsandgrowth