
N Gharahdaghi et al. N Engl J Med 2026;394: 2212-2222. Interleukin-10 Autoantibodies and HLA-DRB1*01:03 in Inflammatory Bowel Disease
Background: “The allele HLA-DRB1*01:03 is the strongest genetic risk factor not only for susceptibility to ulcerative colitis but also for complicated phenotypes, including acute severe ulcerative colitis and an increased likelihood of surgical resection.2-5 However, the underlying pathogenic mechanism linking this HLA allele to disease remains unclear.”
“Neutralizing autoantibodies against interleukin-10 can result in a phenocopy of monogenic defects of interleukin-10 signaling in children and may be associated with inflammatory bowel disease (IBD)…In one child, anti–interleukin-10 titers and disease activity responded to B-cell–depleting anti-CD20 therapy.12“
Methods:
Key findings:
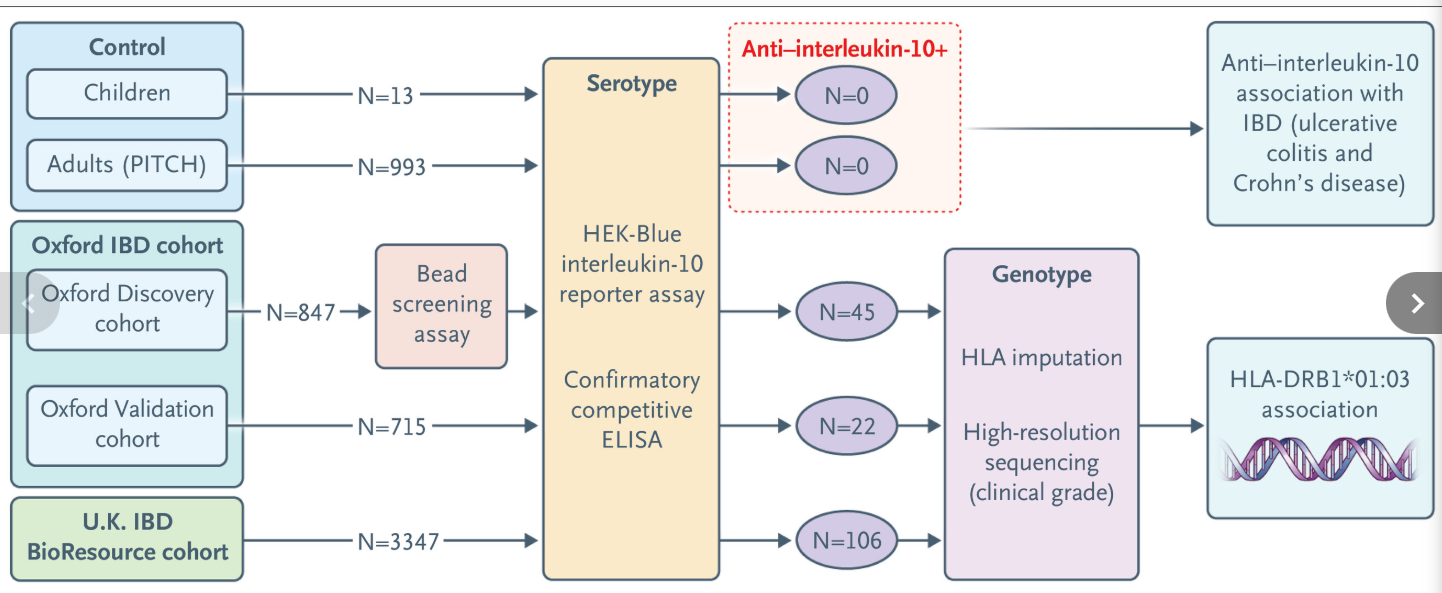
- Interleukin-10–neutralizing autoantibodies were detected in 173 of 4909 patients with IBD (3.5%) and in none of 1006 controls (P<0.001)
- High anti–interleukin-10 activity in serum was associated with a reduction in detectable interleukin-10 and with an exaggerated proinflammatory cytokine response
- Anti–interleukin-10 seropositivity was strongly associated with HLA-DRB1*01:03 on the basis of imputed data from the Oxford cohort (odds ratio, 50.0), the U.K. IBD BioResource cohort (odds ratio, 24.7), and in a high-resolution sequencing analysis of data from the Oxford cohort (odds ratio, 29.5)

Discussion Points:
- “The genetic association between HLA-DRB1*01:03 and anti–interleukin-10 autoreactivity provides mechanistic insight into one of the strongest known genetic susceptibility factors for IBD, with possible diagnostic, prognostic, and therapeutic implications.”
- “Monogenic interleukin-10–signaling defects tend to manifest during infancy with colonic and penetrating disease, poor response to IBD therapies, high inflammatory activity with notably elevated C-reactive protein levels, and a high incidence of postoperative complications.27 It will be informative to establish the extent to which anti–interleukin-10 seropositivity associates with a similar disease pattern.”
- “Our data highlight the need for research into therapeutic maneuvers to reduce anti–interleukin-10 titers — for example, by means of B-cell and plasma-cell depletion (e.g., anti-CD19, anti-CD20, anti-CD38, or CD19 chimeric antigen receptor [CAR] T-cell therapy),29-31 plasma exchange, or blockade of the neonatal Fc receptor.32“
My take: Historically, in younger patients (6 or younger) and those with more severe inflammatory bowel disease, it has been common to evaluate for monogenetic diseases which may require different treatment approaches. For similar reasons, assessing for neutralizing autoantibodies against interleukin-10 is likely to become part of routine care.
Related study: Q Zhang Q, Shakweh E, Sharip M et al. The Lancet Gastroenterology & Hepatology, 2026; 0. Open Access! HLA-DRB1*01:03 in patients with inflammatory bowel disease: a genotype–phenotype association study Key findings:
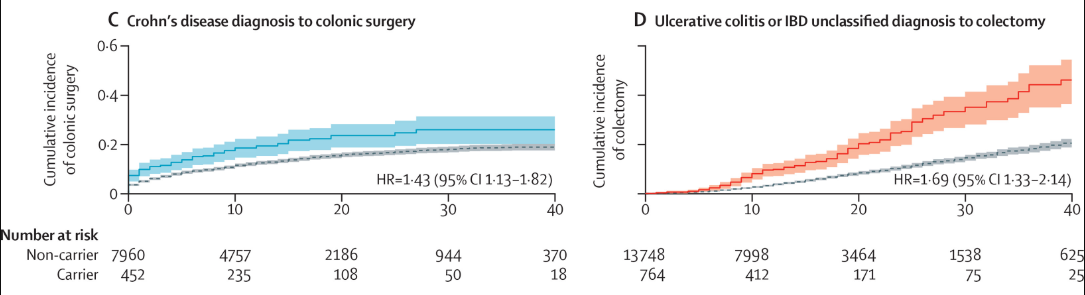
- Among 43,762 patients with IBD (21 839 with Crohn’s disease and 21 923 with ulcerative colitis or IBD unclassified), HLA-DRB1*01:03 carriage was observed in 2009 (4·6%) patients with IBD and associated with multiple severe outcomes …including colonic resection in patients with Crohn’s disease (odds ratio 1·35), colectomy in patients with ulcerative colitis or IBD unclassified (1·99), and perianal disease in both patients with Crohn’s disease (1·65) and patients with ulcerative colitis or IBD unclassified (1·70)

Related blog posts:
- A Medical Wolf in Sheep’s Clothing – Monogenetic Diseases Not So Rare
- Genetic Risk Impacts Severity of Inflammatory Bowel Disease
- Targeted Therapy for Autoinflammatory Very Early Onset Inflammatory Bowel Disease
- Outcomes of Hematopoietic Stem Cell Transplant in Monogenic Inflammatory Bowel Disease
- Immune Dysregulation and Inflammatory Bowel Disease
- How Very Early Onset-Inflammatory Bowel Disease is Different, Plus One
- VEO-IBD -Useful “Position” Paper is Really a Review

