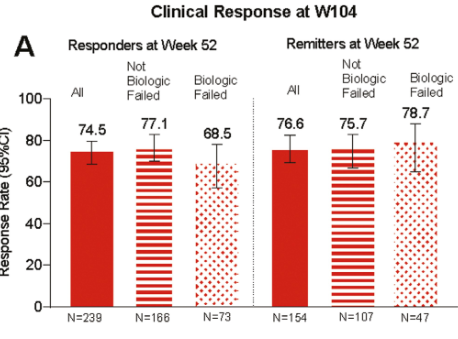
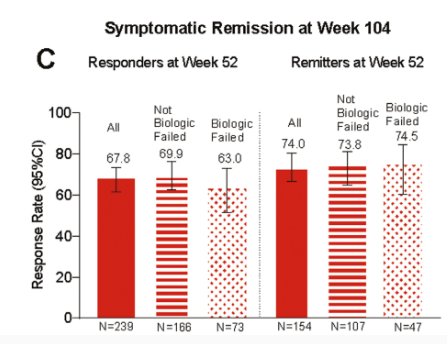
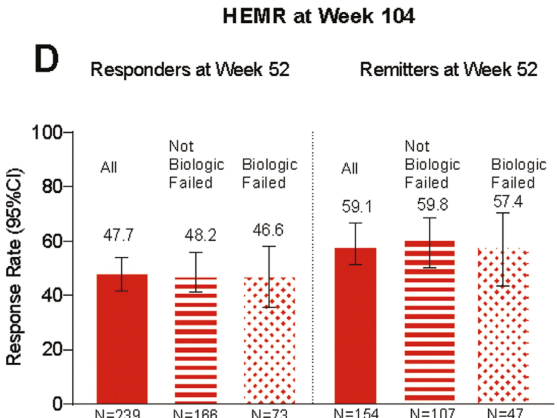
In this LUCENT-3 study, the authors examined response at 2 years among patientswho had response to treatment at 1 year; patients received 200 mg mirikizumab every 4 weeks. The authors stratified patients by induction response and by previous biologic exposure.
Key findings (from Figure 4):
HEMR= histologic-endoscopic mucosal remission
No new safety signals were identified, and the discontinuation rate due to adverse events was 2.8%
My take: It is good to see extended data for mirkizumab. Head-to-head trials, though, are needed to better determine which therapies are most effective.
Of patients not achieving clinical response during 12-week induction, 53.7% achieved response following extended induction (additional 3 doses of IV infusion every 4 weeks)
With “extended induction,” total of 80.3% mirikizumab-treated patients achieved clinical response by W24
Methods: A network meta-analysis (NMA) was conducted to evaluate comparative efficacy of licensed biologics. Phase 3 randomized controlled-trials (RCTs) evaluating biologics approved by the European Medicines Agency or United States Food and Drug Administration as of 31 March 2023 for maintenance treatment of adult patients with moderate-to-severe CD were included, i.e. infliximab (IFX) intravenous (IV) and SC, adalimumab (ADL) SC, vedolizumab (VDZ) IV and SC, ustekinumab (UST) SC, and risankizumab (RZB) SC.
Key findings:
Among 8 comparator arms, IFX SC 120 mg every 2 weeks (Q2W) showed the highest odds ratio (95% credible interval) vs. PBO for clinical remission during the maintenance phase (3.52 [2.18–5.65]).
My take: This meta-analysis shows a favorable response for IFX SC; however, head-to-head trials are needed to really determine which biologic has the highest efficacy.
In this cross-sectional study with 104 children (24 with fatigue), biological parameters (CRP, fecal calprotectin) did not discriminate fatigued from non-fatigued patient
In this multicenter prospective study with 117 patients, the authors examined the success rate of adalimumab (ADA) in patients with CD with an intra-abdominal abscess resolved without surgery.
Key findings:
At W24, the survival rate without abscess recurrence or surgery was 74% (n=87)
Abscess drainage was significantly associated with ADA failure at W24 (odds ratio, 4.18)
My take (borrowed from authors): Provided that the abscess was carefully managed before initiating medical treatment, this study showed the high efficacy of ADA in the short and long term in biologic-naïve patients with CD complicated by an intra-abdominal abscess