- Hydroxychloroquine (HCQ) was used off-label for COVID-19 during the first wave despite the absence of evidence documenting its clinical benefits. A recent study has estimated that it resulted in an increase death rate of 11%. ”The number of hydroxychloroquine related deaths in hospitalized patients is estimated at 16,990 in six countries.” Ref: Open Access! A Pradelle et al. Biomedicine & Pharmacotherapy 2024; 171: 116055. Deaths induced by compassionate use of hydroxychloroquine during the first COVID-19 wave: an estimate
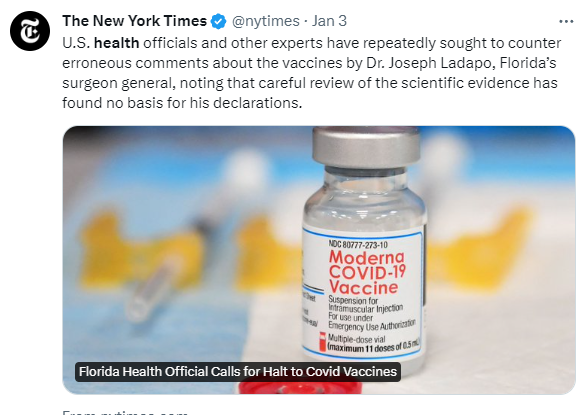
- NY Times 1/3/24: Citing Misinformation, Florida Health Official Calls for Halt to Covid Vaccines
An excerpt:
Florida’s surgeon general on Wednesday called for a halt to the use of Covid vaccines, citing widely debunked concerns that contaminants in the vaccine can permanently integrate into human DNA.
Dr. Ladapo’s latest contention is “very irresponsible,” said John Wherry, a vaccine expert and director of the Institute for Immunology at the University of Pennsylvania. “He has, however, demonstrated a tenuous grasp of science and medicine in general over the course of the pandemic so this is not surprising,” Dr. Wherry said….
For Dr. Ladapo’s claim to be true, humans would need to have an enzyme that can incorporate foreign DNA into their genomes. “We don’t have one,” said Dr. Eric Rubin, a member of the F.D.A.’s vaccine advisory committee and the editor in chief of the New England Journal of Medicine.
My take: The first article estimates the number of deaths due to the bad advice of using hydroxychloroquine. Perhaps in a few years, researchers will be able to calculate the number of deaths and hospitalizations that occur due to the bad advice of Florida’s surgeon general.
Related blog posts:
- Florida Narrative Ignoring Inconvenient Data with COVID-19 Vaccine Safety
- Florida Surgeon General Hinders Public Health
- Prevalence of Rome IV Functional Bowel Disorders in Adults (US, UK, Canada) & Largest Study to Date on Hydroxychloroquine for COVId-19
- Drunk Driving Deaths Fall, Unexpected Problem Related to “Frozen” Movie, and Hydroxychloroquine Trial
- Eric Topol to Stephen Hahn/FDA: “Tell the Truth or Resign”