ECF Brown et al NEJM 2025; 392: 1148-51. Partnerships between Pharmaceutical and Telehealth Companies — Increasing Access or Driving Inappropriate Prescribing?
This recent commentary discusses the upsides and pitfall of online platforms launched by pharmaceutical companies that direct users to websites run by telehealth companies.
An excerpt:
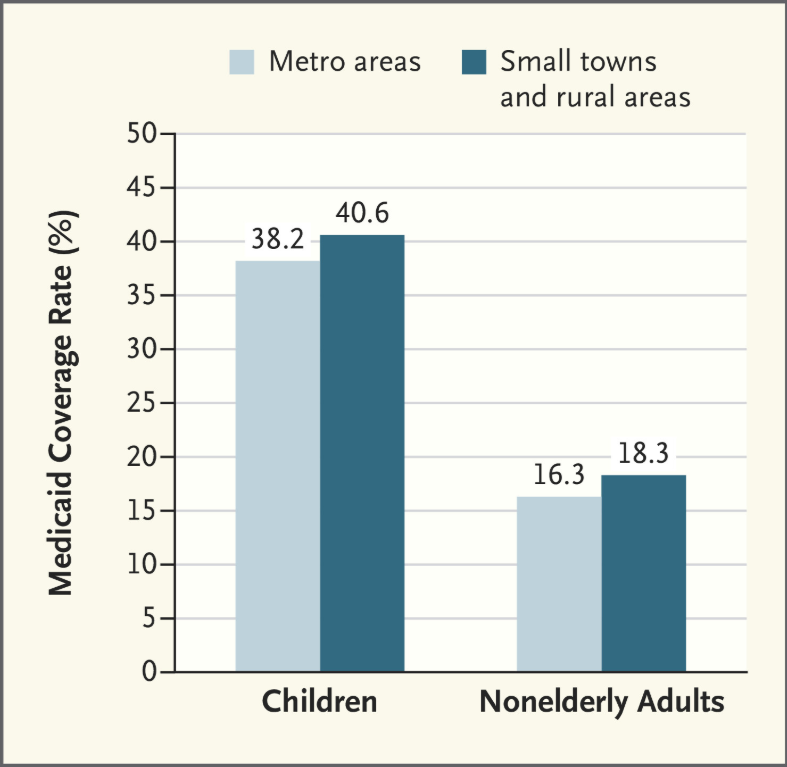
Proponents highlight the potential for pharmaceutical–telehealth partnerships to facilitate access to prescriptions for some patients, such as those in rural areas…. Virtual consultations can be cheaper and less time-consuming for patients than in-person appointments. For stigmatized conditions such as obesity, patients may be more likely to seek care …
But partnerships between drug and telehealth companies have prompted concerns as well…about the risks these arrangements pose in terms of inappropriate prescribing, inadequate follow-up care, and unnecessary spending on brand-name medications.1 There is also concern that telehealth advertisements, including those on social media, may be misleading, since they sometimes lack disclosures of a product’s risks and contraindications.
The key law governing these relationships in the United States is the federal Anti-Kickback Statute (AKS). The AKS is intended to prevent and penalize the use of financial incentives for patient referrals or other arrangements that encourage clinicians to provide inappropriate or unnecessary health care, thereby increasing government expenditures…
Under the AKS, a pharmaceutical company cannot compensate a telehealth company or its affiliated clinicians on the basis of the number or monetary value of prescribed products. Nor may a telehealth company pay a pharmaceutical company for making patient referrals…
The OIG also noted several characteristics of telehealth arrangements that heighten the risk of an AKS violation. These characteristics include patient recruitment using targeted advertising (including on social media), insufficient patient evaluation or follow-up, and steering of patients toward specific treatments without adequate consideration of clinical appropriateness or alternatives…
More information about the nature of financial arrangements between pharmaceutical and telehealth companies should be reported. Such reporting could be mandated as part of an expansion of the Physician Payments Sunshine Act.
My take: There needs to be closer scrutiny of the relationship between pharmaceutical companies and affiliated telehealth companies. While the online telehealth partnershps improve access, the current set up is likely to promote inappropriate care.