Link: The Struggle is Real (44 secs)


Link: The Struggle is Real (44 secs)
Correction: Yesterday’s post was updated after an astute observation from one of my colleagues (Jordan) to note that the pictured instrument was in fact a harpsichord rather than a piano. A harpsichord’s sound is derived from plucking a string whereas a piano’s sound comes after a hammer strikes a chord.
——–
JW Chen et al. AJG 2023; 118: 1334-1343. Interrater Reliability of Functional Lumen Imaging Probe Panometry and High-Resolution Manometry for the Assessment of Esophageal Motility Disorders
Thanks to Ben Gold for this reference. Also, congratulations to Jose Garza -our motility specialist and a coauthor of this study.
15 motility specialists completed their interpretation of 40 consecutive HRM (high resolution manometry) and 40 FLIP (functional lumen imaging probe panometry) studies. All were part of a FLIP study group. Key findings:
My take: This is a reassuring study indicating that with the most consequential esophageal findings, there is excellent agreement among motilist interpretation. Previous studies of colonic manometry, in contrast, have found much lower levels of agreement.
Related blog posts:

G Polanco, et al. JPGN Reports 4(3):p e322, August 2023. Open Access! Delayed Hypersensitivity Reaction to Infliximab Due to Mammalian Meat Allergy
Briefly noted: Case report of a 17 yo with Crohn’s disease who developed urticaria and pruritus approximately 6 hours after her very first infliximab infusion; the patient was diagnosed with Alpha-Gal and responded to change to adalimumab which is not glycosylated with alpha-gal.
Related blog post: Nonanaphylactic Alpha-Gal and Chronic Gastrointestinal Symptoms

L Pace, K McGoogan. JPGN Reports 4(3):p e327, August 2023. Open Access! Vaping Induced Severe Erosive Esophagitis
This case report describes a 17 yo with sore throat, odynophagia chest pain, and dysphagia associated with vaping. His symptoms resulted in hospitalization and he underwent an EGD on day 4 after symptoms had not improved with multiple empiric therapies.
EGD findings included .
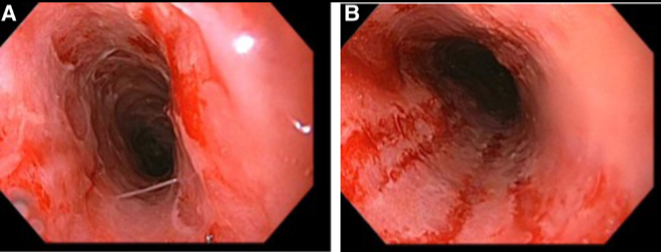
My take: When adolescent patients present with esophageal symptoms, inquiring about exposure to vaping along with medications known to cause pill-esophagitis, is worthwhile.
Related blog post: Review: Infectious Esophagitis
HM Horita et al. J Pediatr 2023; 261: 113549. Open Access! Development of a Medical Complexity Score for Pediatric Aerodigestive Patients
Methods: The authors in this study developed a 7-point medical complexity score . One point was assigned for each comorbid diagnosis in the following categories: airway anomaly, neurologic, cardiac, respiratory, gastrointestinal, genetic diagnoses, and prematurity. A retrospective chart review was conducted of patients (n=234) seen in the aerodigestive clinic who had ≥2 visits between 2017 and 2021.
Improvements were followed in the Functional Oral Intake Scale (FOIS)–assigned by aerodigestive feeding therapists.6 The FOIS scale is as follows:
Key findings:

My take: While the complexity score did correlate with likelihood of progressing with oral feedings, it appears that this score is unnecessary as likelihood of progressing is mainly related to two factors: neurological comorbidities and airway anomalies.
Related blog posts:
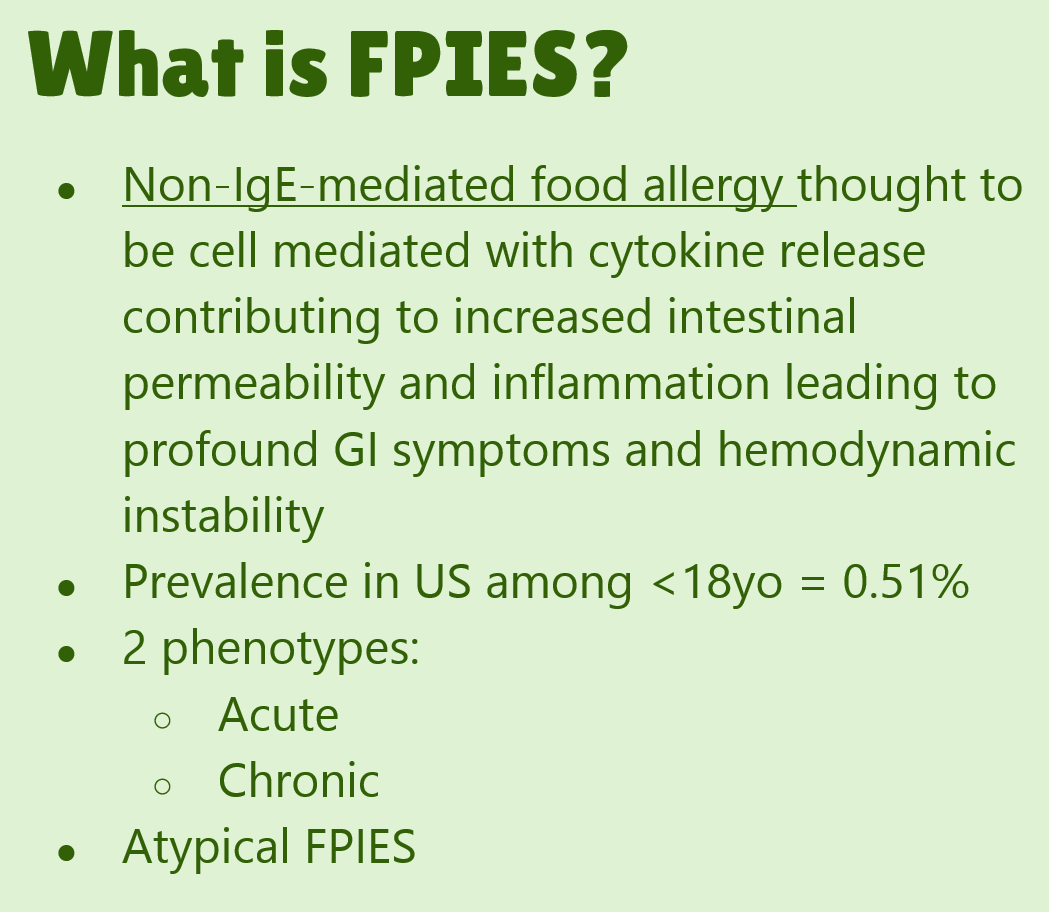
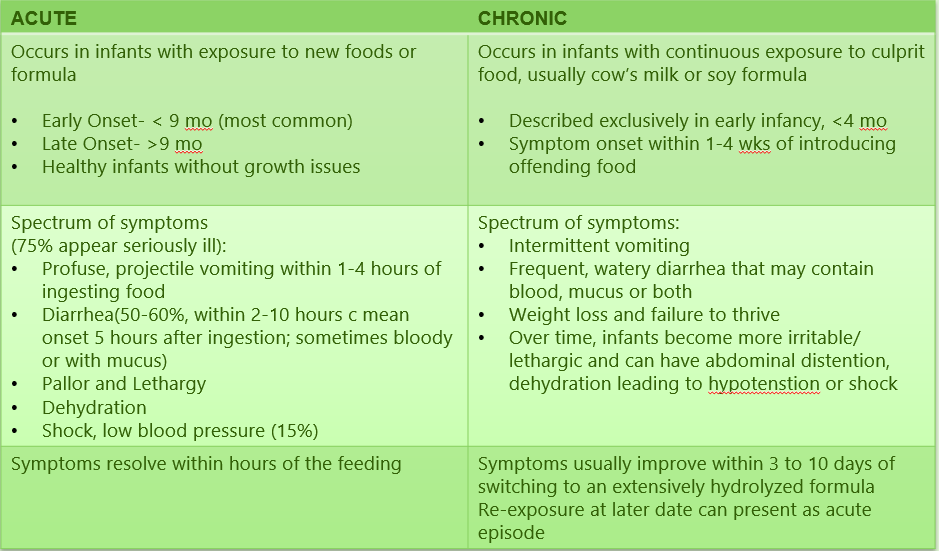
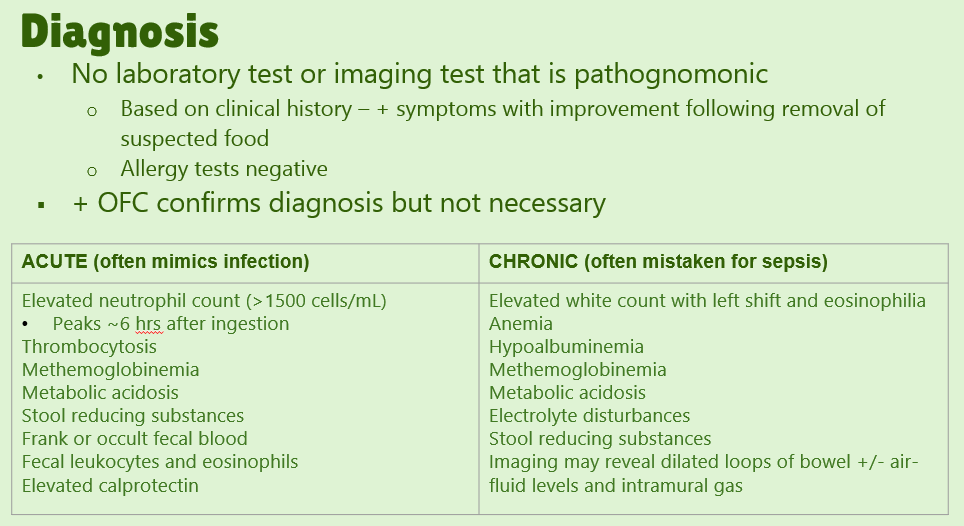
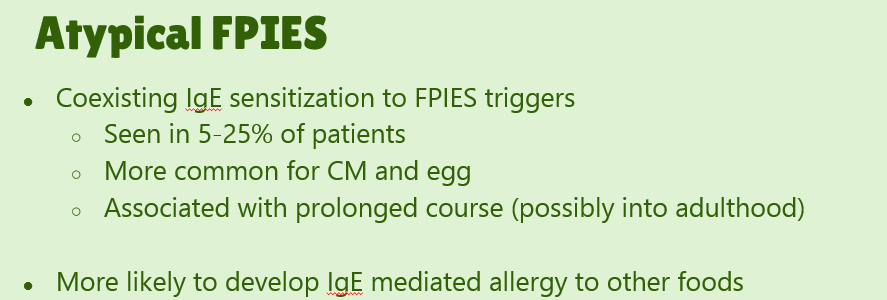
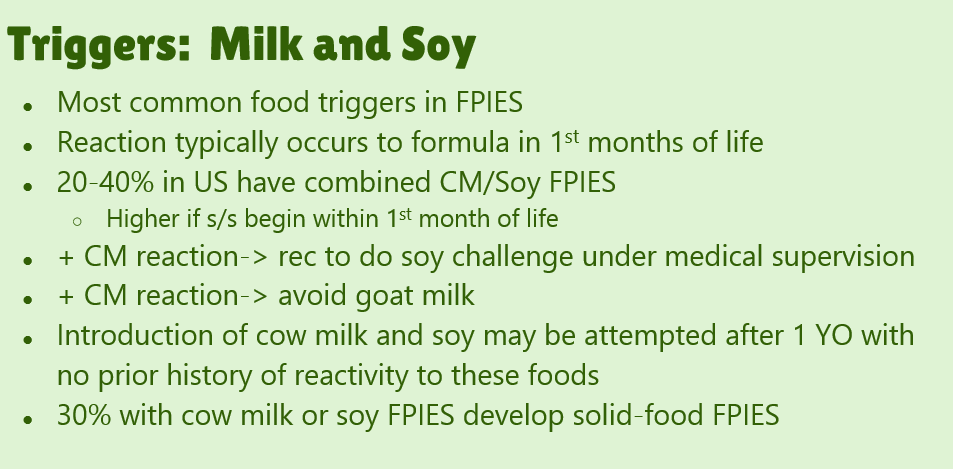
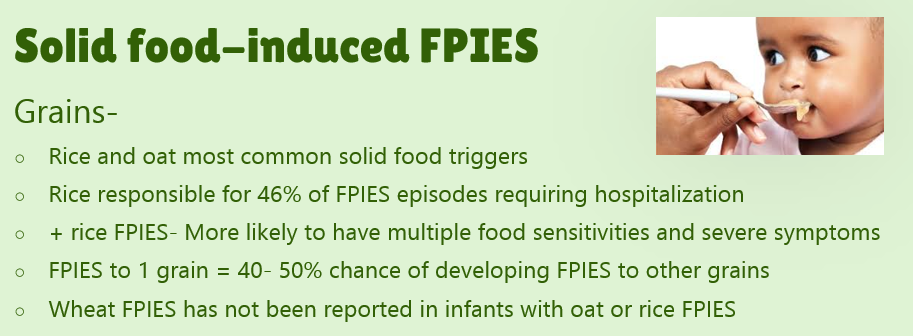
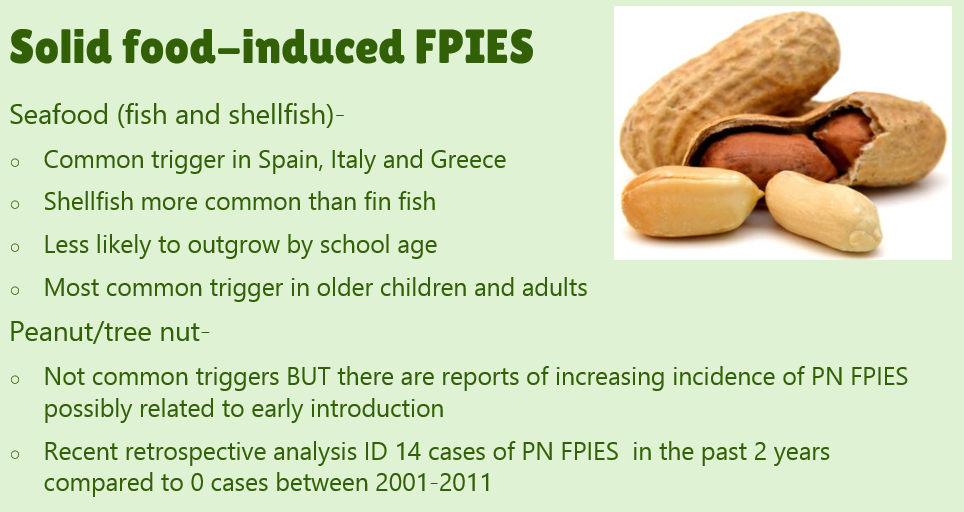
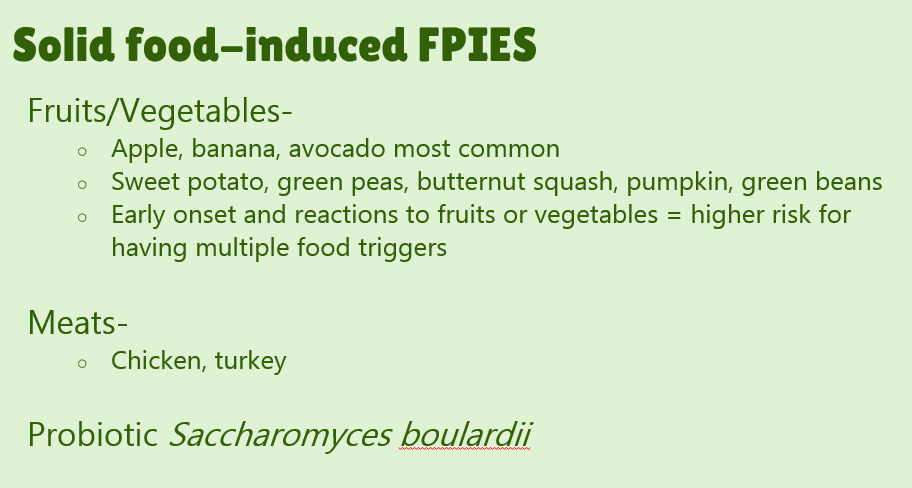
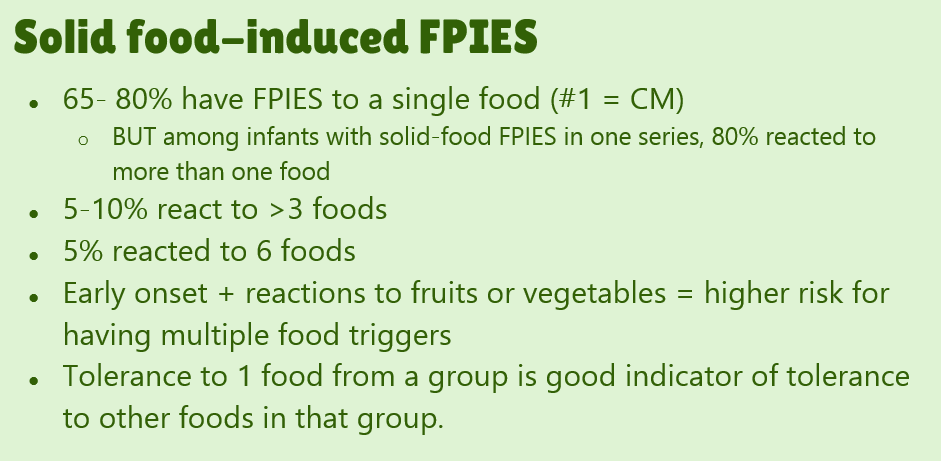
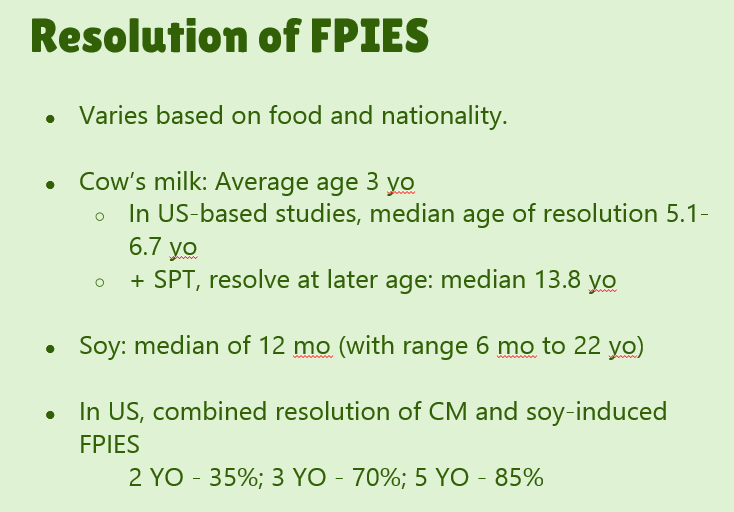
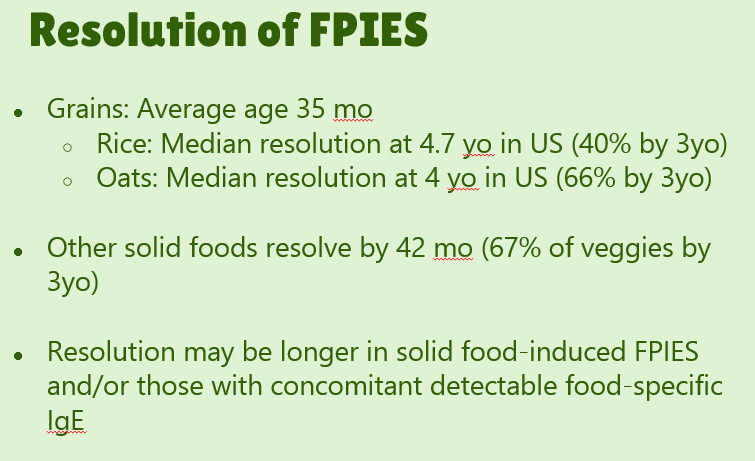
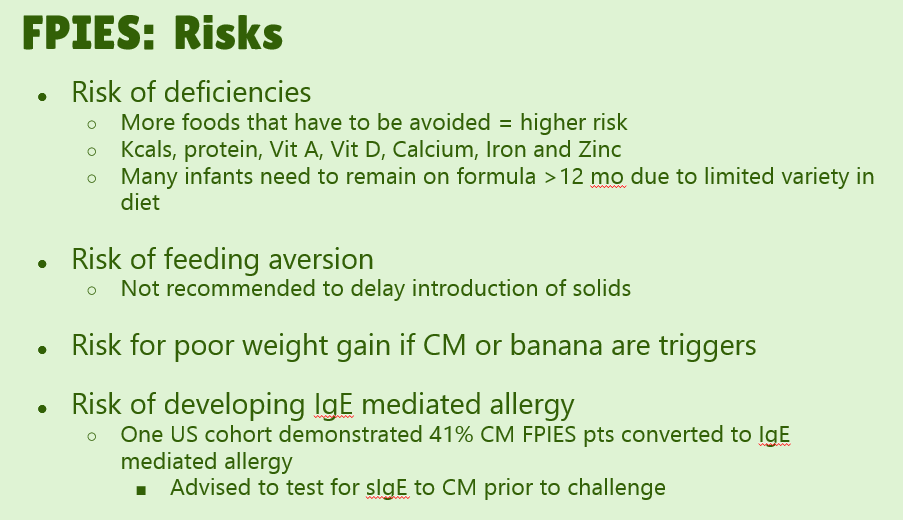
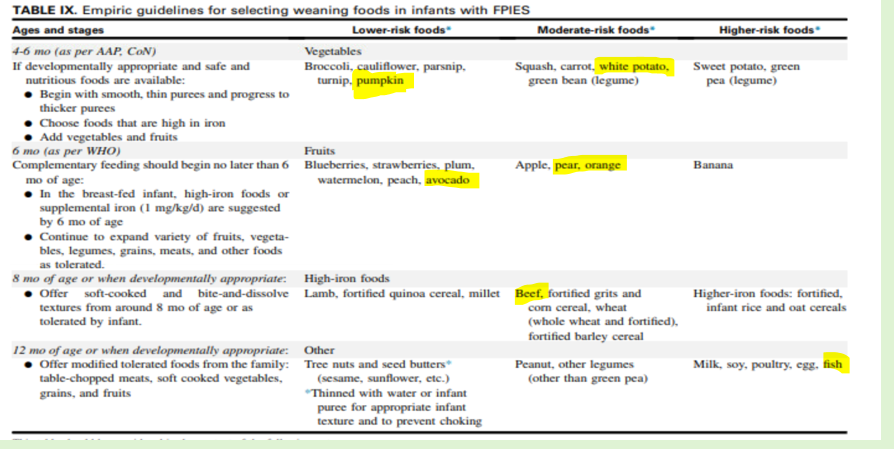
Our excellent nutritionist, Bailey Koch, recently gave our group a terrific update on FPIES. Bailey is part of the medical advisory board for THE FPIES Foundation, as is Dr. Benjamin Gold from our group. Here are many of the slides from her lecture.


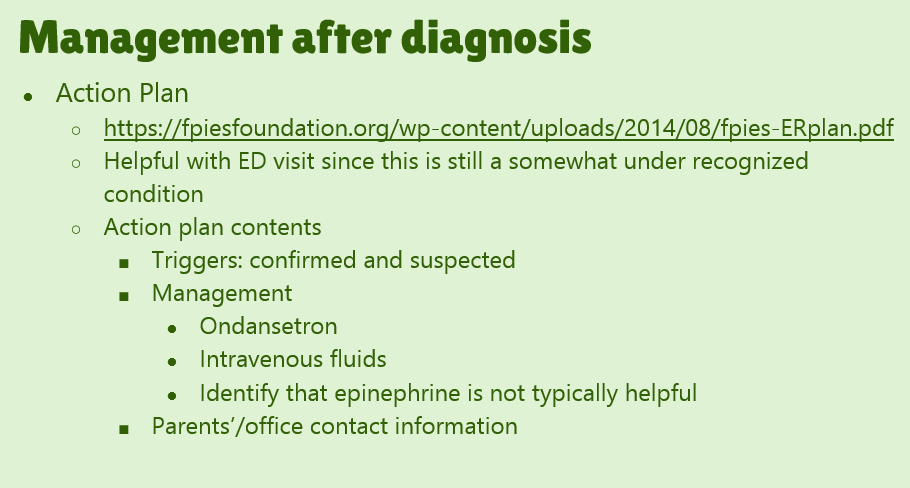
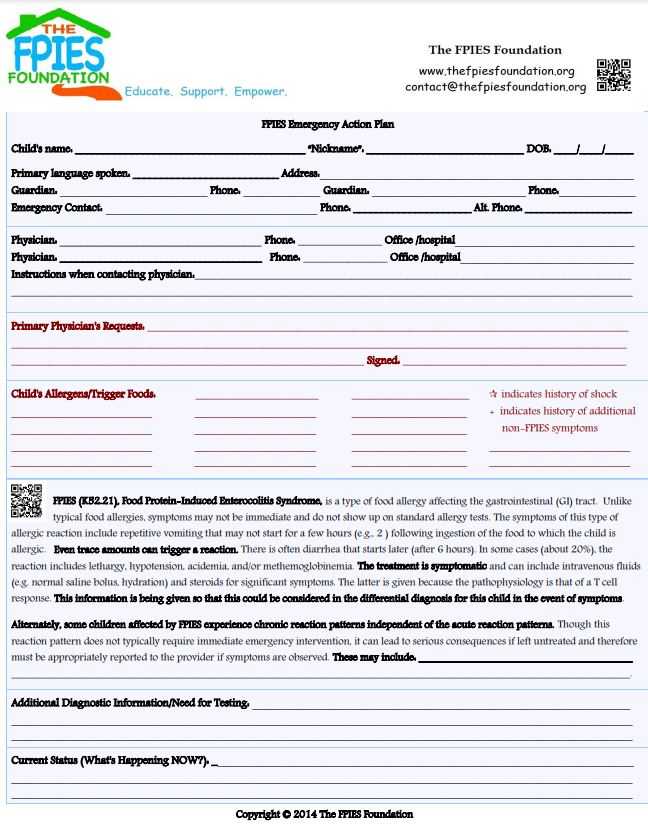
Link: FPIES foundation action plan sheet:


Nowak-Węgrzyn A, Chehade M, Groetch ME, et al. Open Access: International consensus guidelines for the diagnosis and management of food protein-induced enterocolitis syndrome: Executive summary-Workgroup Report of the Adverse Reactions to Foods Committee, American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol. 2017;139:1111-26.
Related blog posts:
From FPIES 2017 Guidelines:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
BR Lee et al. J Pediatr 2023; 261: 113551. A Comparison of Pathogen Detection and Risk Factors among Symptomatic Children with Gastroenteritis Compared with Asymptomatic Children in the Post-rotavirus Vaccine Era
Patients (<11 yrs old) with acute gastroenteritis (AGE, n=2503) and healthy controls (HC, n=537) old enrolled in the New Vaccine Surveillance Network study between December 2011 to June 2016. Key findings:
This study shows substantial improvement in rotavirus infections with a drop from 26% in detection prior to vaccine era to 6% afterwards.
My take: These muliplex molecular assays are quite useful and have improved our ability to determine underlying infections. This is particularly useful in children with underlying diseases (eg. IBD, malignancy). However, this report serves as a cautionary note that many pathogens, including C diff and E coli, are frequently identified with PCR assays in healthy children
Related blog posts:
In 2022, 892 infants died in Georgia, an increase of 116 from prior year. About 7 infants dying for every 1000 births. AJC 11/1/23: CDC: Georgia’s infant mortality increase is among the worst in U.S.


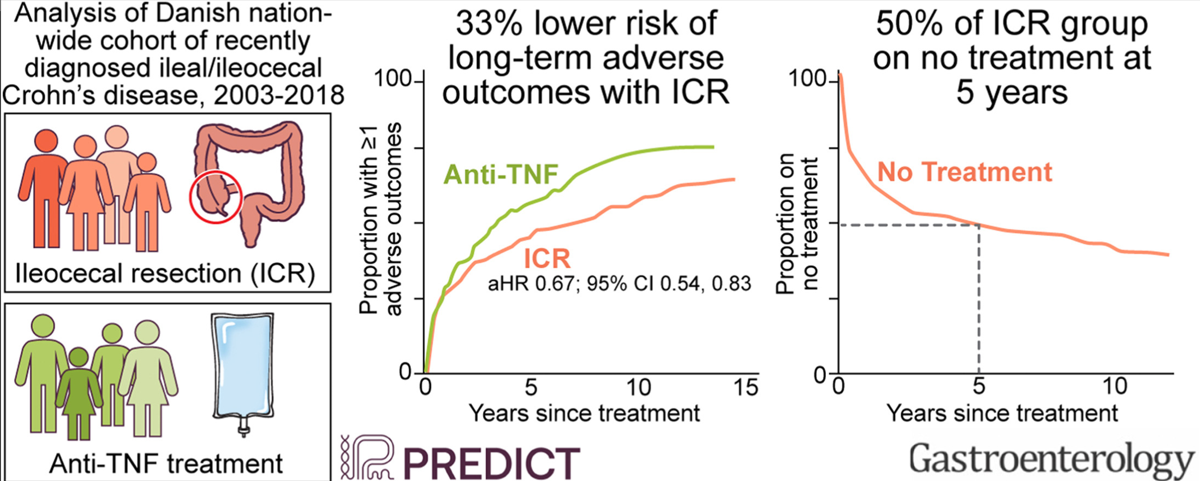
M Agrawal et al. Gastroenterol 2023; 165: 976-985. Open Access! Early Ileocecal Resection for Crohn’s Disease Is Associated With Improved Long-term Outcomes Compared With Anti-Tumor Necrosis Factor Therapy: A Population-Based Cohort Study
In this study from Denmark (2003-2018) using the Danish National Patient and Prescription Registries, the role of early ileocecal resection (CR), n=581, was compared with anti-TNF treatment, n=698. The primary outcome was a composite of ≥1 of the following: CD-related hospitalization, systemic corticosteroid exposure, CD-related surgery, and perianal CD. Only 178 patients (13.9%) were less than 17 years old. ICR cohort had surgery within 5 months of diagnosis in 85%, and in all within 1 yr of diagnosis. Key findings:
The authors note that their cohort had infrequent complicated disease: “Before ICR, 21% were diagnosed with a stricture, ileus, internal fistula, or abscess, indicative of complicated CD and representative of the real world. In contrast, only 1.7% in the anti-TNF group had complicated CD.”
My take: This study suggests that ICR may be a reasonable option in many cases of Crohn’s disease at an earlier stage rather than reserved for only those with refractory disease and complications. However, in pediatric patients, I would be more reluctant to start with a surgical approach given even longer time frame in which further surgery could be needed.
Related blog posts:
Yesterday’s post was meant to be published on Halloween –will need to fire my editor.
———-
One of the highlights of NASPGHAN’s annual meeting is the Year in Review lecture. Sandeep Gupta, the editor of JPGN, provided a fantastic review. Here are some of the slides:











FA Hanna et al. JPGN 2023; 77: 505-511. Thiopurines Maintenance Therapy in Children With Ulcerative Colitis: A Multicenter Retrospective Study
In this retrospective study with 133 children (2008-2019), typical dosing of thiopurines: azathioprine 2-2.5 mg/kg/day and 6-mercaptopurine 1.5 mg/kg/day. Patients with previous or concomitant treatment with 5-ASA were allowed in the study. 62% (n=83) of the cohort had pancolitis. Key Findings:
In their discussion, the authors make several points regarding efficacy and safety of thiopurines.
My take: In the U.S., it appears that thiopurine monotherapy, and even combination therapy, in pediatrics with IBD is used infrequently. Anti-TNF therapy with therapeutic drug monitoring is used routinely in patients if a 5-ASA is ineffective or not a good option. This article is a reminder that thiopurines are still a reasonable option. This would have been a good opportunity for a commentary in JPGN to add some context to this article regarding the role of these agents.
AGA guidelines for moderate-to-severe ulcerative colitis: “In adult outpatients with moderate to severe UC in remission, AGA makes no recommendation in favor of or against using biologic monotherapy or tofacitinib rather than thiopurine monotherapy for maintenance of remission.”
Related blog posts:


