VG Clark et al. Gastroenterol 2024; (in press). DOI:https://doi.org/10.1053/j.gastro.2024.06.028 Fazirsiran for Adults with Alpha-1 Antitrypsin Deficiency Liver Disease: A Phase 2 Placebo Controlled Trial (SEQUOIA)
Key findings:
At Week 16, least-squares mean percent declines in serum Z-AAT concentration were −61%, −83% and −94% with fazirsiran 25/100/200 mg, respectively, versus placebo (all P< .0001)
Efficacy was sustained through Week 52. At post-dose liver biopsy, fazirsiran reduced median liver Z-AAT concentration by 93% compared with an increase of 26% with placebo
All fazirsiran-treated patients had histological reduction from baseline in hepatic globule burden
Portal inflammation improved in 5/12 and 0/8 patients with baseline score >0 in the fazirsiran and placebo groups, respectively
Histological METAVIR score improved by >1 point in 7/14 and 3/8 patients with fibrosis >F0 at baseline in the fazirsiran and placebo groups, respectively
My take: This is an exciting development for patients with A1AT-associated liver disease. Longer duration data is needed to confirm whether fazirsiran will be a useful therapeutic agent for A1AT deficiency. If effective, selecting patients who benefit from treatment will need to be determined.
Recently, Dr. William Balistreri presented a review of some of the biggest advances in pediatric hepatology this past year on the Bowel Sounds Podcast (with the award-winning hosts).
He discussed the following:
IBAT inhibitors which are a game-changer for pruritic cholestatic disorders like Alagille syndrome. By reducing itching, it may help many avoid liver transplantation
HCV medications which usually result in a cure with typical therapy courses running 8-12 weeks
Emergence of a new treatment, Fazirsiran, for alpha-one antitrypsin deficiency (see blog post below)
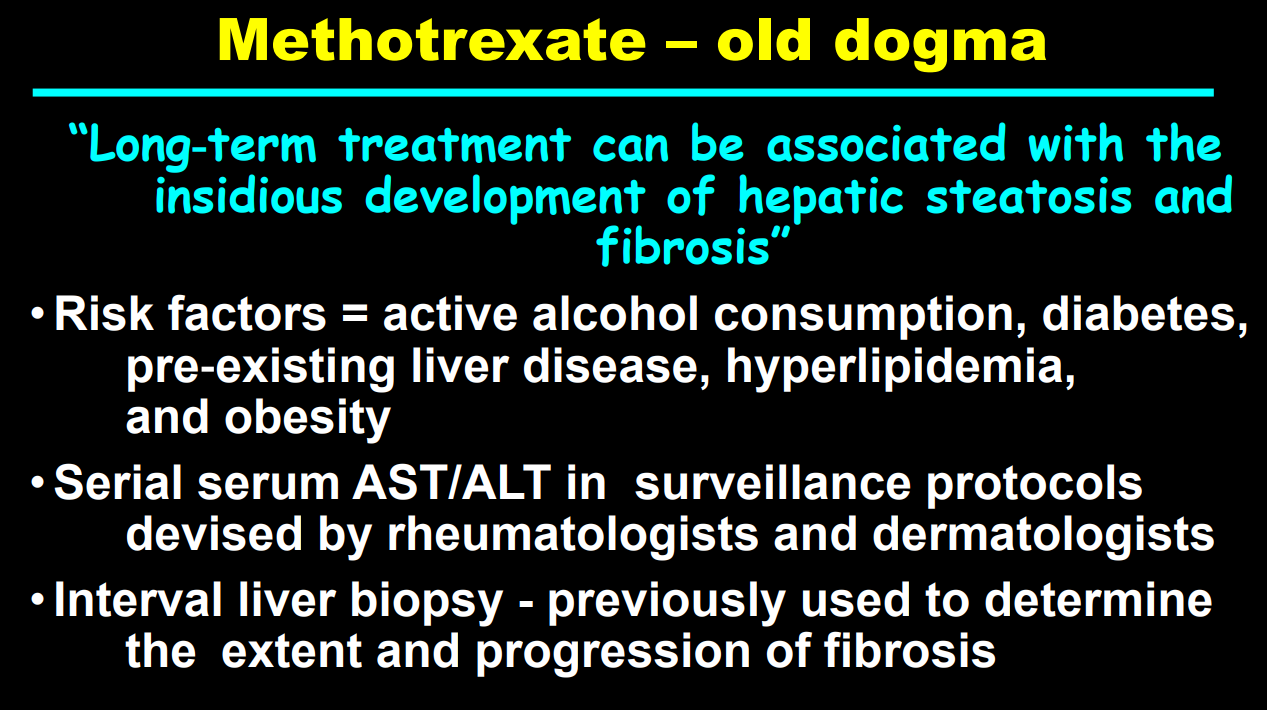
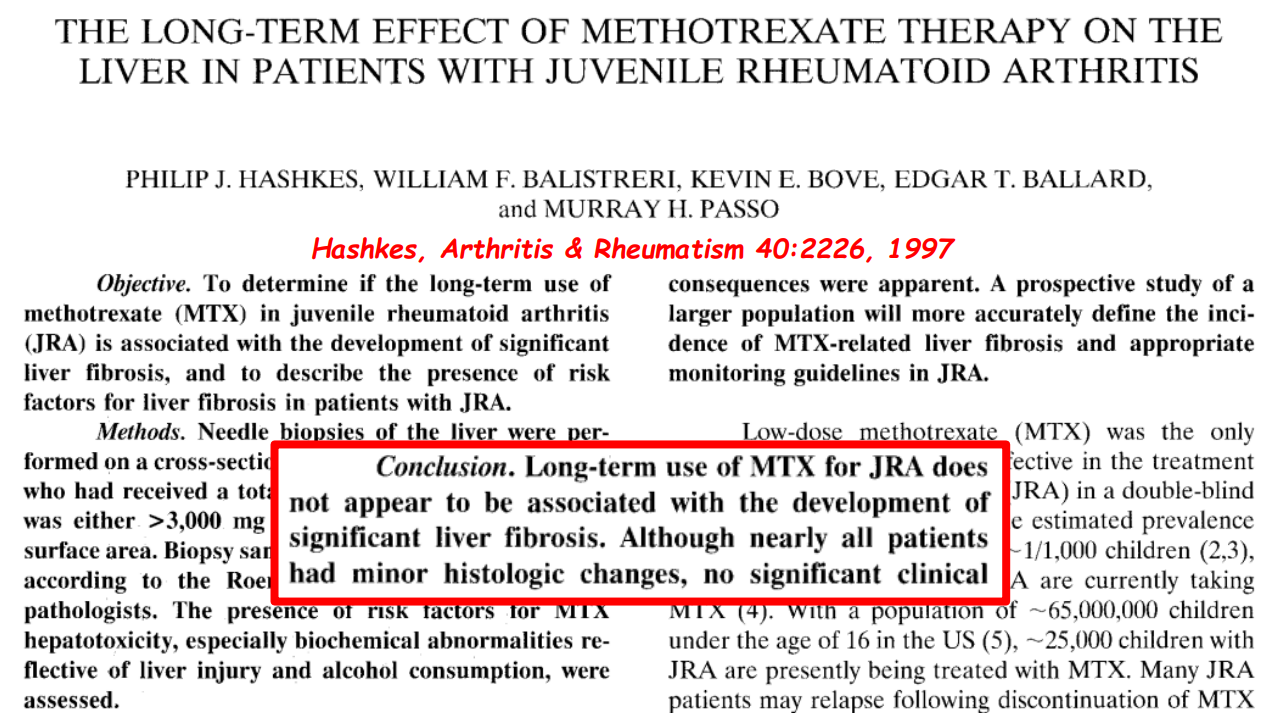
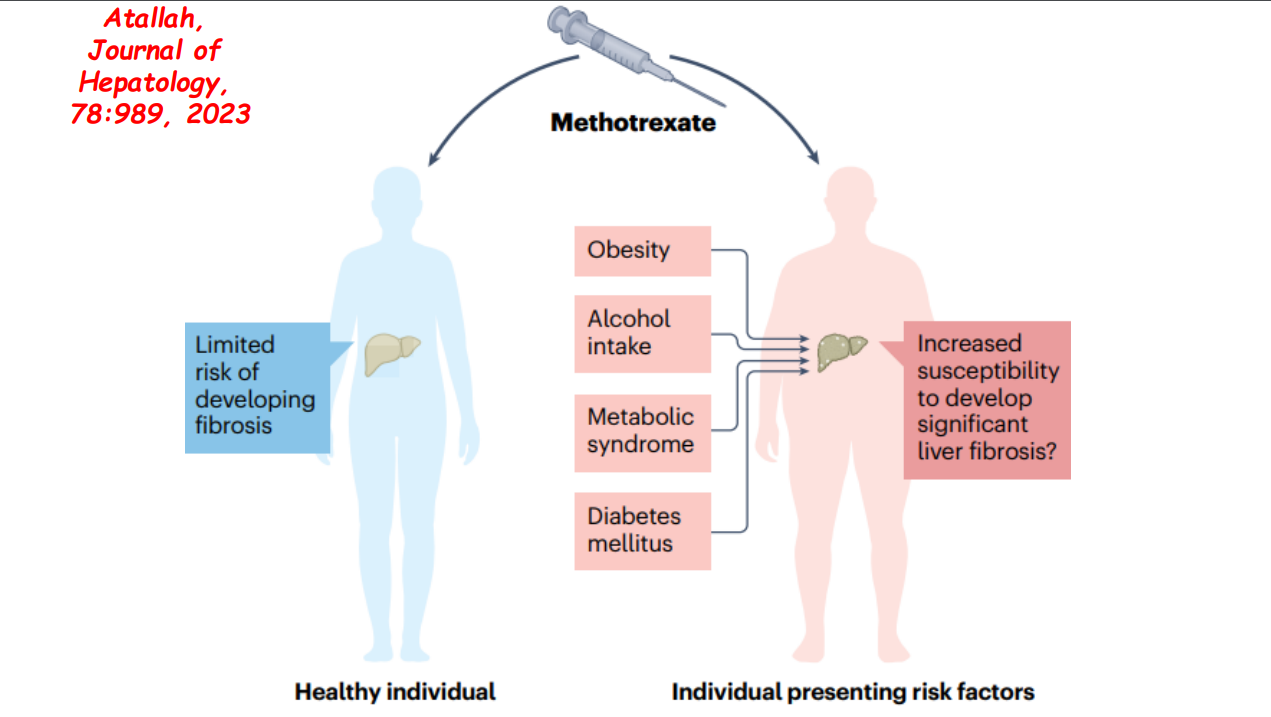
More data showing the good liver safety of methotrexate in individuals without preexisting liver disease. Dr. Balistreri and colleagues showed pediatric patients with JRA did not develop liver fibrosis/clinical liver disease in 1997.
Alpha-1-Antitrypsin Deficiency (review May 2020). 35% of adults with ZZ genotype show clinically-significant liver fibrosis. Risk factors for advanced fibrosis: male gender, metabolic syndrome/obesity, and alcohol consumption.
Background: “Z-AAT accumulation has been correlated with liver fibrosis, a finding that suggests that reducing Z-AAT production may improve hepatic phenotypes…RNA interference (RNAi) is a naturally occurring cellular mechanism that regulates gene expression. Fazirsiran (previously ARO-AAT) is an investigational RNAi therapeutic that contains a synthetic, double-stranded, small interfering RNA duplex conjugated to N-acetylgalactosamine, which binds to the hepatocyte asialoglycoprotein receptor to facilitate endosomal uptake and intracellular delivery…Fazirsiran causes degradation of AAT and Z-AAT messenger RNA, thus reducing both AAT and Z-AAT protein synthesis in hepatocytes.” Fazirsiran has already shown effectiveness in a mouse model and had an adequate safety profile in a phase 1 study with healthy volunteers.
Methods: Phase 2, open-label, multicenter trial enrolled adults with the PI ZZ genotype and liver fibrosis. They received fazirsiran subcutaneously on day 1 and week 4 and then every 12 weeks
Key findings:
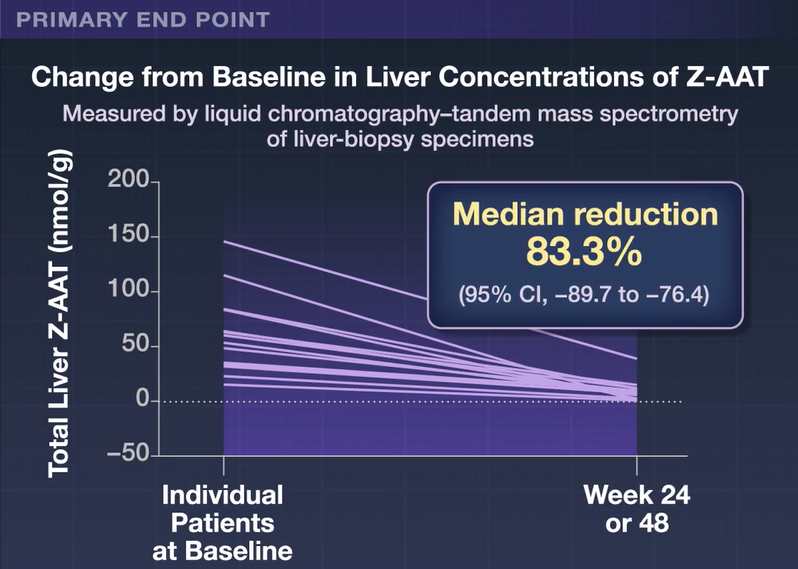
All the patients had reduced accumulation of Z-AAT in the liver (median reduction, 83% at week 24 or 48)
Fibrosis regression was observed in 7 of 15 patients and fibrosis progression in 2 of 15 patients after 24 or 48 weeks
There were no adverse events leading to trial or drug discontinuation. Four serious adverse events (viral myocarditis, diverticulitis, dyspnea, and vestibular neuronitis) resolved. Most common adverse events were arthralgia and transient increase in creatinine kinase (each in 4 patients). It was noted that there was a gradual decrease in mean FEV1 through week 52 but no evidence that this was due to fazirsiran treatment.
The authors note that reduction in Z-AAT accumulation is expected to yield clinical benefit since the liver is a regenerative organ.
My take: This is an exciting development for patients with AAT-associated liver disease but a larger, placebo-controlled treatment trial with longer duration is needed to confirm whether fazirsiran will be a useful therapeutic agent for AAT deficiency.
After reviewing this study, I contacted one of the authors (Dr. Teckman) to find out about the status of pediatric studies. His response:
A larger, phase III study is going to start enrolling soon (for adults) to better define the risks, benefits, dose, length of therapy and patient selection which will hopefully lead to full FDA approval. The next phase of fazirsiran for adults will have many sites and St Louis will be one. Patients are welcome to contact me.
Trials with fazirsiran for children are being designed. Time frame 1-3 years. Other drugs are also close to opening studies for kids, as well.
Several other drugs that appear promising for AAT are also in phase I, II, soon III. That’s great news. I commonly refer patients to “clinicaltrials.gov” but they can contact me or the Alpha-1 Foundation for information.
All patients should read the extensive and very informative patient literature on the Alpha-1 Foundation web site; www.alpha1.org.
All patients should enroll in the Alpha-1 Registry. This is a scientific, IRB approved registry which is non-interventional and does not commit patients to anything, but which will permit them to be contacted and kept informed about potential trials. It is for anyone who carries any number of many abnormal genotype; ZZ, SZ, MZ, null, etc.
All eligible people who are anywhere near a site should be enrolled in the Childhood Liver Disease Research Network; www.childrennetwork.og. This is a non-interventional, NIH- sponsored network which studies pediatric liver disease. ZZ and SZ patients ages 0 years to 25 years can enroll. You do not need to change doctors or care sites. Many patients stay with their docs they have but contribute to the study once a year.
Related blog posts:
Alpha-1-Antitrypsin Deficiency (review May 2020). 35% of adults with ZZ genotype show clinically-significant liver fibrosis. Risk factors for advanced fibrosis: male gender, metabolic syndrome/obesity, and alcohol consumption.