WJ Sandborn et al. Gastroenterol 2022; 162: 1650-1664. Open Access: Guselkumab for the Treatment of Crohn’s Disease: Induction Results From the Phase 2 GALAXI-1 Study
Background: Guselkumab, a selective p19 interleukin-23 antagonist, is approved for the treatment of plaque psoriasis and psoriatic arthritis.
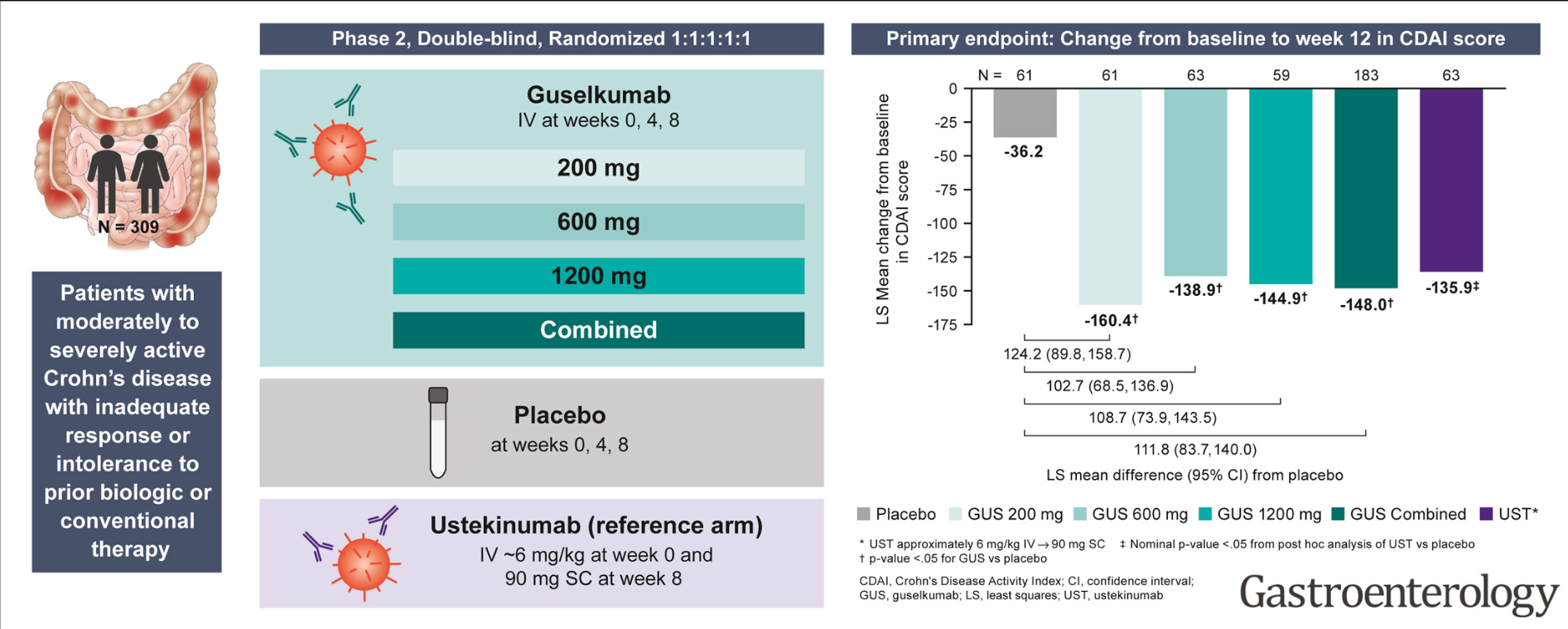
Methods: GALAXI-1, a phase 2, double-blind, placebo-controlled study, randomized patients with moderate to severe Crohn’s disease 1:1:1:1:1 to intravenous guselkumab 200 mg, 600 mg, or 1200 mg at weeks 0, 4, and 8; intravenous ustekinumab approximately 6 mg/kg at week 0 and 90 mg subcutaneously at week 8; or placebo. n=309 with ~50% having disease refractory to prior biologics
Key findings:
- At week 12, significantly greater reductions in Crohn’s Disease Activity Index from baseline (least squares means: 200 mg: –160.4, 600 mg: –138.9, and 1200 mg: –144.9 vs placebo: –36.2; all, P < .05) and significantly greater proportions of patients achieved clinical remission in each guselkumab group vs placebo
- Improvement compared to placebo was evident as early as week 4
- Safety event rates were generally similar across treatment groups
My take: This is an exciting time for practitioners taking care of patients as there are an increasing number of pharmacologic and dietary treatments for inflammatory bowel disease. With guselkumab, there may be an overlapping mechanism with ustekinumab which targets IL-12/23.
Related blog post: Emerging Data on Risankizumab for Crohn’s Disease