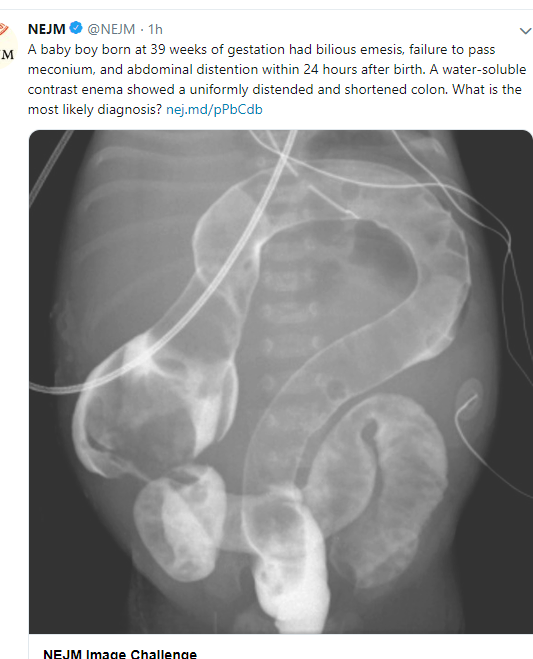
Hirschsprung’s disease with total colonic aganglionosis
Related blog posts:

Hirschsprung’s disease with total colonic aganglionosis
Related blog posts:
Our hospital switched to a new rectal suction biopsy device. This ~ 9 minute YouTube video, rbi2 rectal suction, explains how it is assembled and provides pointers on its use –thanks to Steven Liu for this link.

I have no financial stake in this product.
Briefly noted:
RJ Meinds et al Clin Gastroenterol Hepatol 2015; 13: 1801-07. In this retrospective analysis (1975-2011) of 529 rectal suction biopsies (RSBs) from 441 patients, the authors note lower sensitivity for RSB in infants <40 days.
From Table 3:
Bottomline: This study may need to be replicated due to improvements in biopsy analysis (eg. calretinin); however, in the first 40 days of life, RSBs are more often inconclusive and/or false-negatives. The use of anorectal manometry may be helpful.
Related blog posts:

Two articles provide some insight into endoscopic interventions on both ends of the gastrointestinal tract.
In the first article (JPGN 2014; 59: 608-11), the authors retrospectively studied 11 children who received mitomycin-C concurrently with endoscopic dilatation for the treatment of anastomotic strictures after esophageal atresia repair. Key finding: 8 of 11 achieved resolution of their strictures, 2 remained with stenosis, and 1 needed surgical correction. However, the authors found no benefit of mitomycin C in the resolution of the strictures compared with endoscopic dilatation alone in historical controls (n=10). In fact, in this small study, the control group patients had fewer endoscopic dilatations (3.7 vs. 5.4 dilatations per patient) and 9 of 10 achieved stricture resolution.
In the second article (JPGN 2014; 59: 604-08), the authors retrospectively reviewed the outcome of children (n=33) with surgically-treated Hirschsprung’s disease (HD) who were treated with intrasphincteric Botox injections for obstructive symptoms. In these children with median age of first Botox injection was 3.6 years; a median of 2 injections were given. 26 (79%) had had a transanal endorectal pull-through. Key finding: initial improvement was noted in 76% and “good/excellent” long-term response was evident in 52% (Table 2).
Bottomline: Botox therapy appears helpful for non-relaxing sphincters in HD whereas mitomycin-C remains an unproven therapy for esophageal strictures.
Also briefly noted: JPGN 2014; 59: 674-78. “Use of cyproheptadine in young children with feeding difficulties and poor growth in a pediatric feeding program.” n=127. Of the 82 who took cyproheptadine regularly, 96% reported a positive change in feeding behaviors and there was a significant improvement in weight gain.
Also, with regard to stooling problems, Sana Syed (Emory GI fellow) pointed out a useful website that emphasizes proper positioning for functional constipation: squattypotty.com. While the website promotes their product to provide proper foot support (with elevation), there are other ways to get a similar result. As noted previously (“Poo in You” Video | gutsandgrowth) proper positioning can help a lot.
Related posts:
Last night, a symposium on “Genetic Testing and the Future of Pediatric Gastroenterology” sponsored by Children’s Healthcare of Atlanta took place. The speakers included Dr. Ben Gold from our pediatric GI group (GI Care for Kids), Dr. Saul Karpen and Dr. Subra Kugasthasan (Emory), and Dr. Robert Heuckeroth (CHOP).
This blog entry has abbreviated/summarized the presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. All of the speakers had terrific presentations.
GI Genetic Testing –Subra Kugathasan
Reasons for genetic testing:
Examples in current medicine:
Who/When to test?
Take-home point: “All GI diseases have genetic testing in future.” Testing for highly selected patients for gene defects can be accomplished with gene panel and if negative, whole exome testing.
Related blog posts:
Liver: Cholestatic & Metabolic Diseases of Infants and Children —Saul Karpen
Potential areas for genetic testing:
“Why bother…they all get transplanted anyway…” According to Dr. Karpen, this view needs to be reconsidered.
Neonatal cholestasis:
PFIC: Progressive Familial Intrahepatic Cholestasis
Biliary Atresia:
NAFLD: Associated with increased mortality compared with matched controls. Patients develop thicker atherosclerotic plaques. PNPLA3 gene identified as a susceptibility gene for NAFLD and is highly prevalent in Hispanic populations. Similarly, PNPLA3 has been associated with NASH in Italian populations. If you have this genotype, this increases risk of liver fat in the face of increased sugar consumption.
Transplant medicine: Deoxyguanosine Kinase Deficiency (DGUOK) –rapid sequencing for this gene pretransplant –If positive, should not be transplanted. These individuals have systemic disease that cannot be cured with liver transplantation.
Who/When for genetic testing?: DGUOK in liver failure patients, and in infants without diagnosis after liver biopsy/exclusion of A1AT
Take-home message: Genetic testing has a role in pediatric liver disease and it is affordable.
Related blog posts:
GI –Single Microbes to the Microbiome and GI Disease —Ben Gold
Key points:
Why the microbiome is so important/more pointers:
Helicobacter pylori -evidence of H pylori as far back as 60,000 years ago and has evolved with humans. H pylori may have helped provided a positive immune response in children and adults.
Bottomline: Human genetic diseases may be heavily influenced by the 300 trillion bacteria and their genes; these bacteria are susceptible to environmental disease.
Related blog posts:
Genetic Basis of Motility —Robert Heuckeroth
Hirschsprung’s disease:
Pseudoobstruction genetic basis– a number of genes identified, including ACTG2 (smooth muscle actin gene). If you understand etiology, this may lead to prevention and treatment.
Take-home message: Currently biggest problem with genetic testing, especially with motility disorders, is identifying genetic defect of unknown significance. Thus, testing needs to be done as part of research studies.
Related blog posts:
Previously this blog noted the emergence of calretinin immunohistochemisty (What is calretinin? | gutsandgrowth). Now, more data has been published indicating that calretinin reduces inconclusive rectal biopsies for the diagnosis of Hirschsprung’s disease (JPGN 2014; 58: 603-07).
The authors analyzed data retrospectively for 45 patients prior to the use of calretinin and 42 patients after calretinin introduction.
Key finding: 37.8% (17 of 45) of patients had inconclusive rectal biopsies prior to use of calretinin compared with 11.9% (5 of 42) after including calretinin immunohistochemistry.
If you are wondering what these are, you may want to review a recent consensus statement (JPGN 2013; 57: 677-86).
This ‘practical guide’ discusses Hirschsprung’s disease, intestinal neuronal dysplasia, chronic intestinal pseudo-obstruction, ultrashort segment Hirschsprung’s disease, hypoganglionosis, and ganglioneuromatosis in MEN 2B.
Most of the focus is on Hirschsprung’s disease including the intricacies of diagnosis, clinical presentation, and genetics. While the authors do mention the PHOX2B gene and others, there is not a discussion of Ondine’s curse (Congenital central hypoventilation syndrome and Hirschsprung’s …). One point that I think is important (but not discussed in the above reference) in patients who have Ondine’s curse and Hirschsprung’s is determining whether a family member may have a milder phenotype that could still place them at risk for sudden death (eg. after a simple sedation procedure).
Related blog post:
