An important recent study (B Kerur et al. Clin Gastroenterol Hepatol 2018; 16: 1467-73 & editorial C Ballengee S Kugasthasan 1398-1400) examined the impact of biologic therapies on Crohn’s disease progression and need for surgery in 1442 children (age, ≤16 y) between 2002-14. This study examined data from the Pediatric Inflammatory Bowel Disease Collaborative Research Group registry.
Key findings:
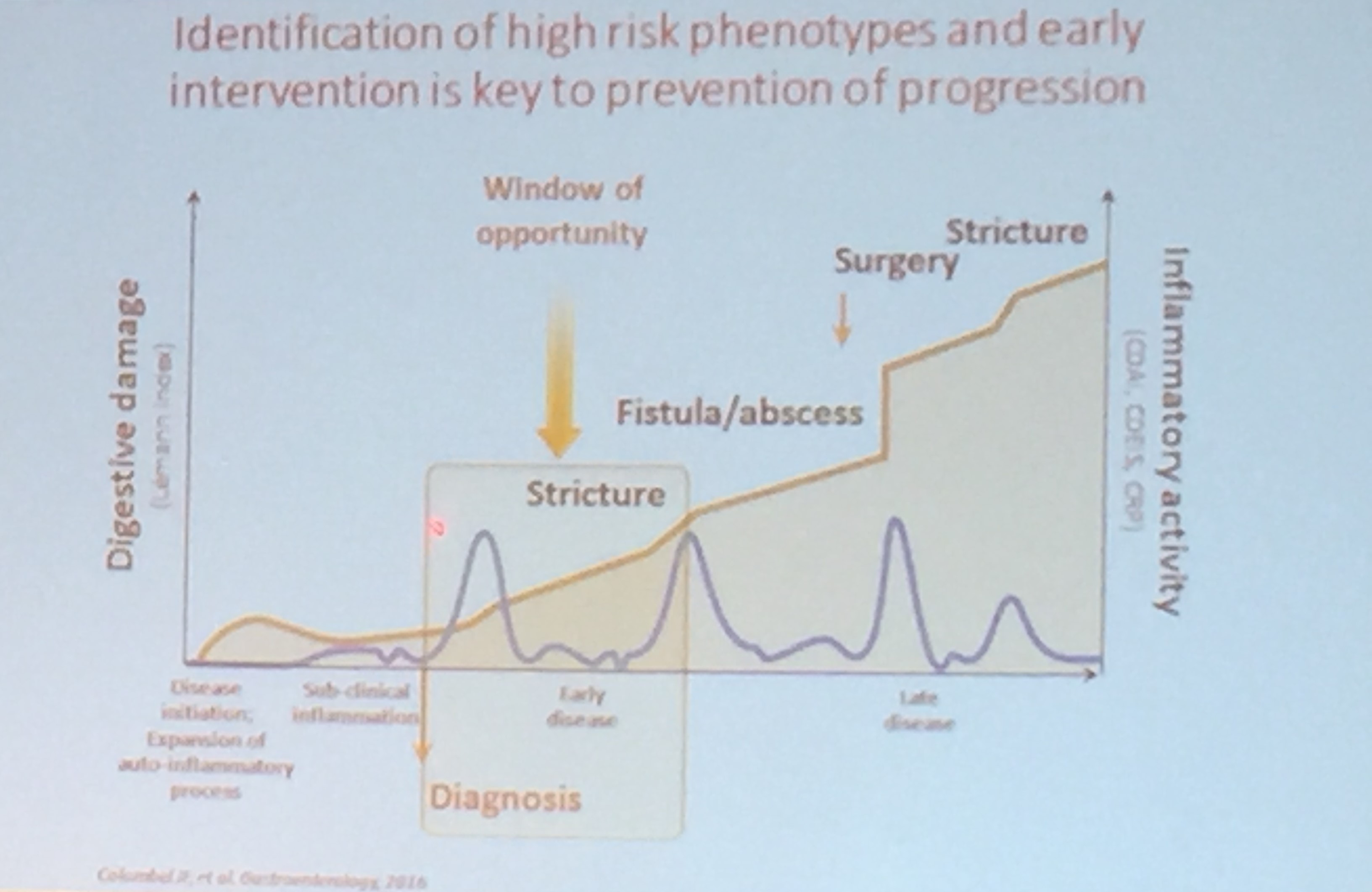
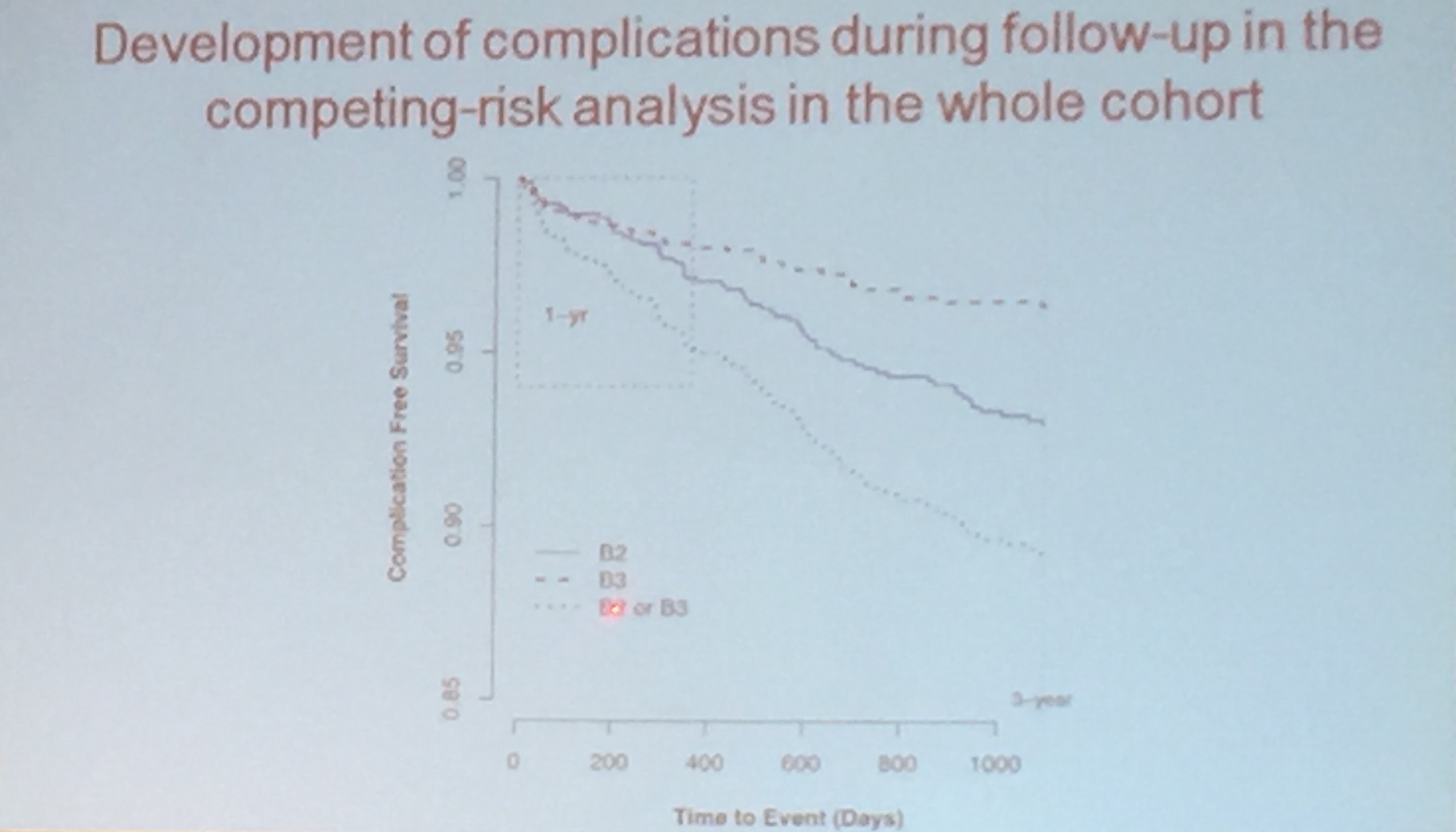
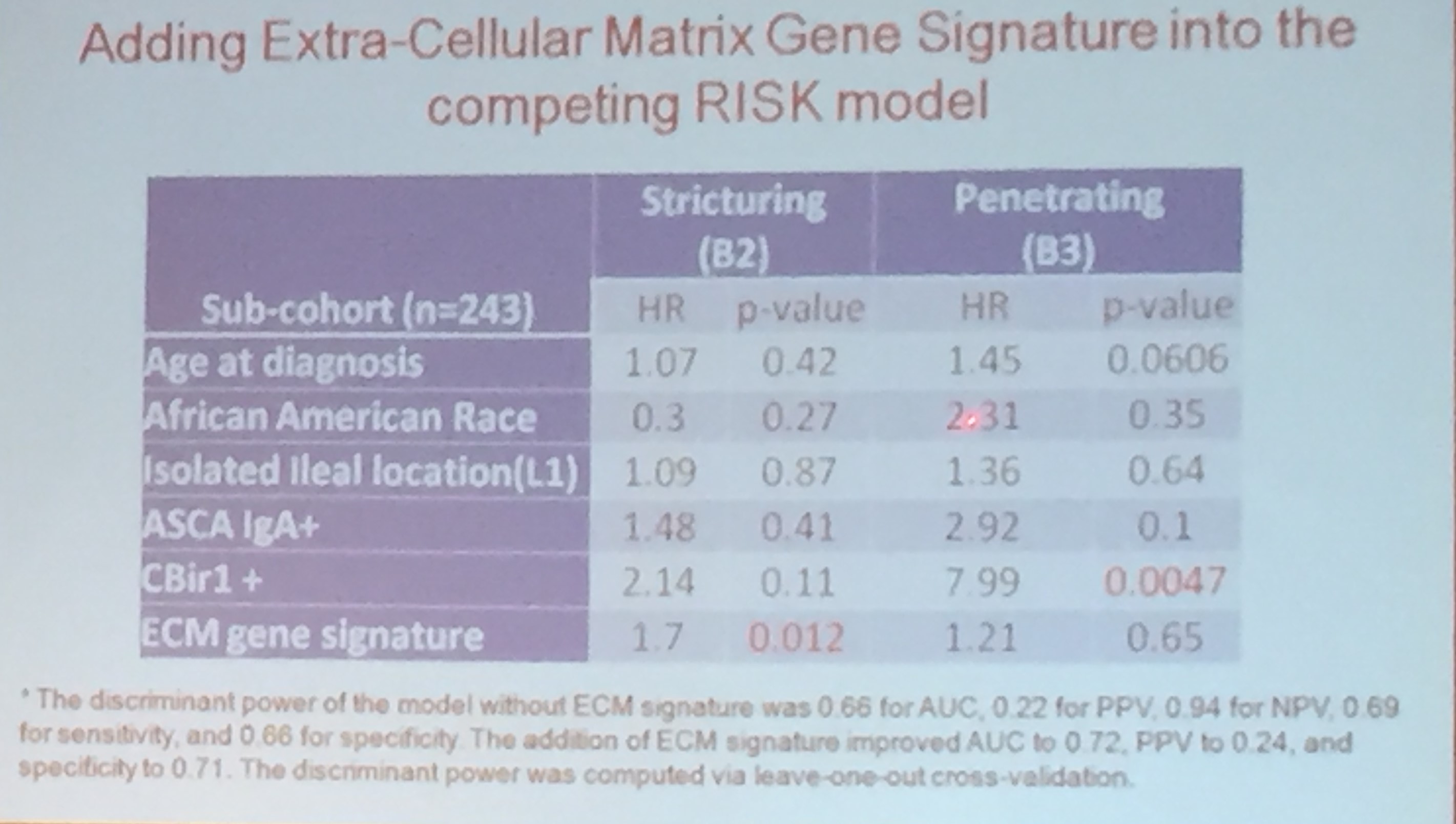
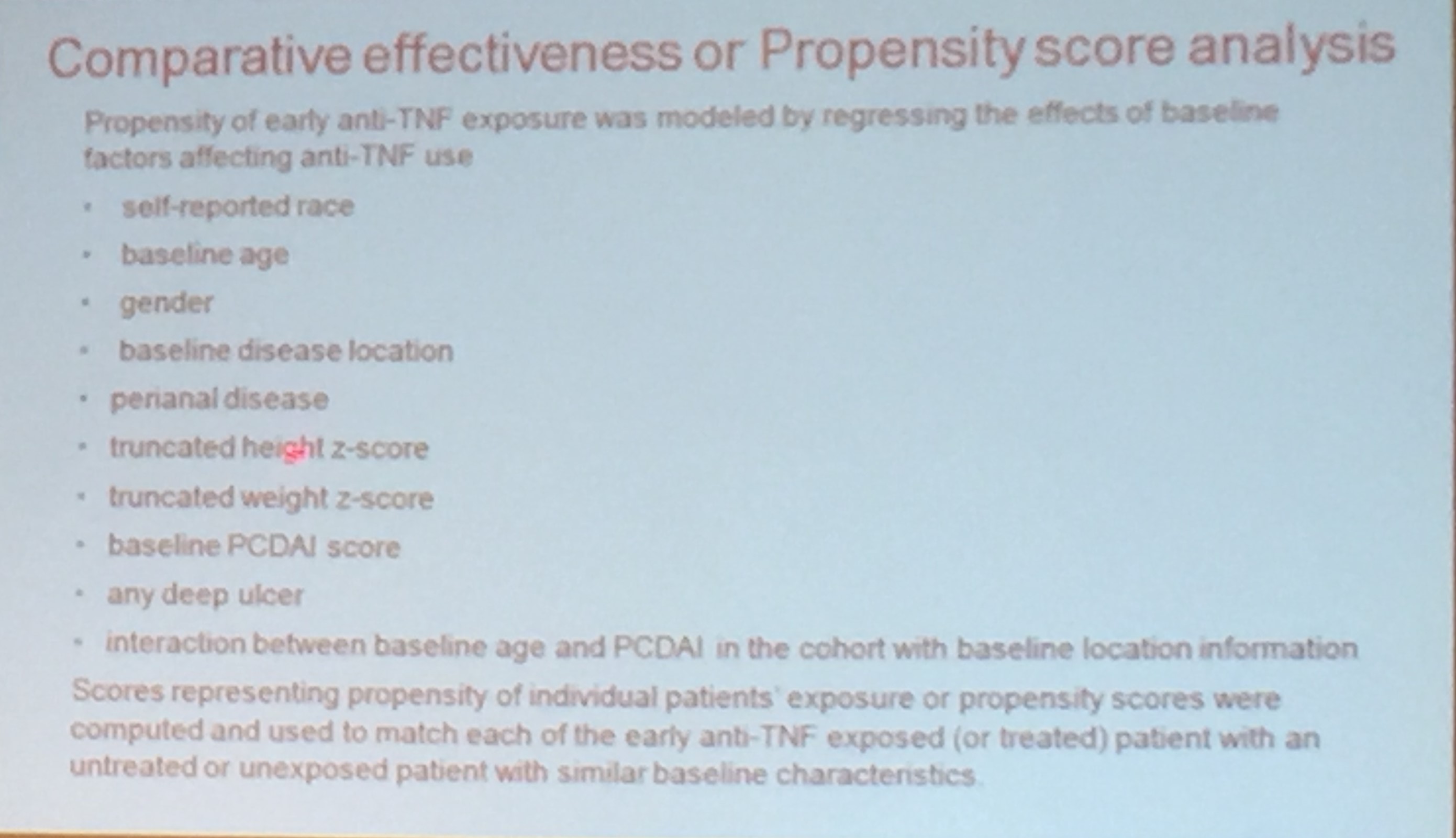
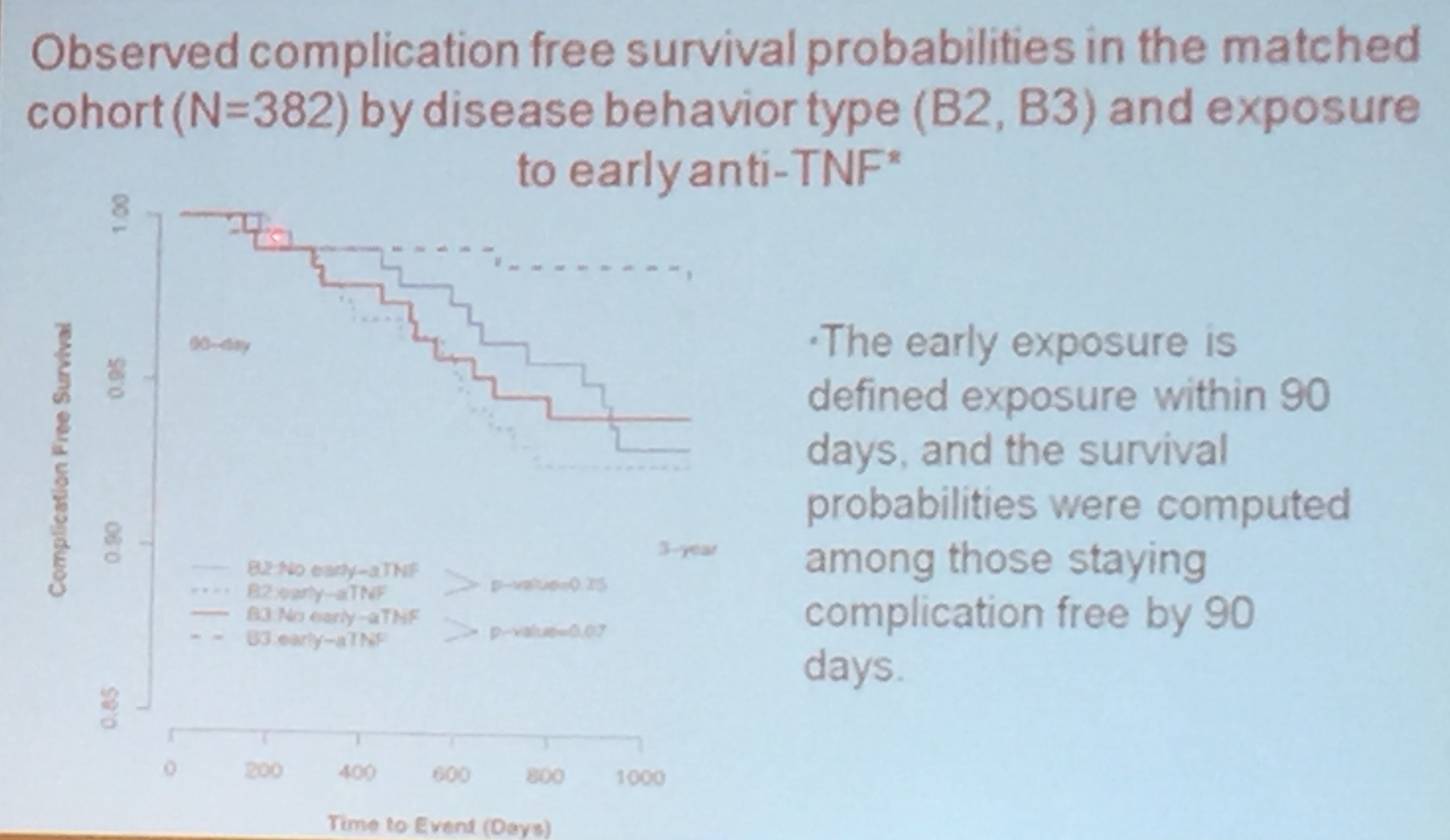
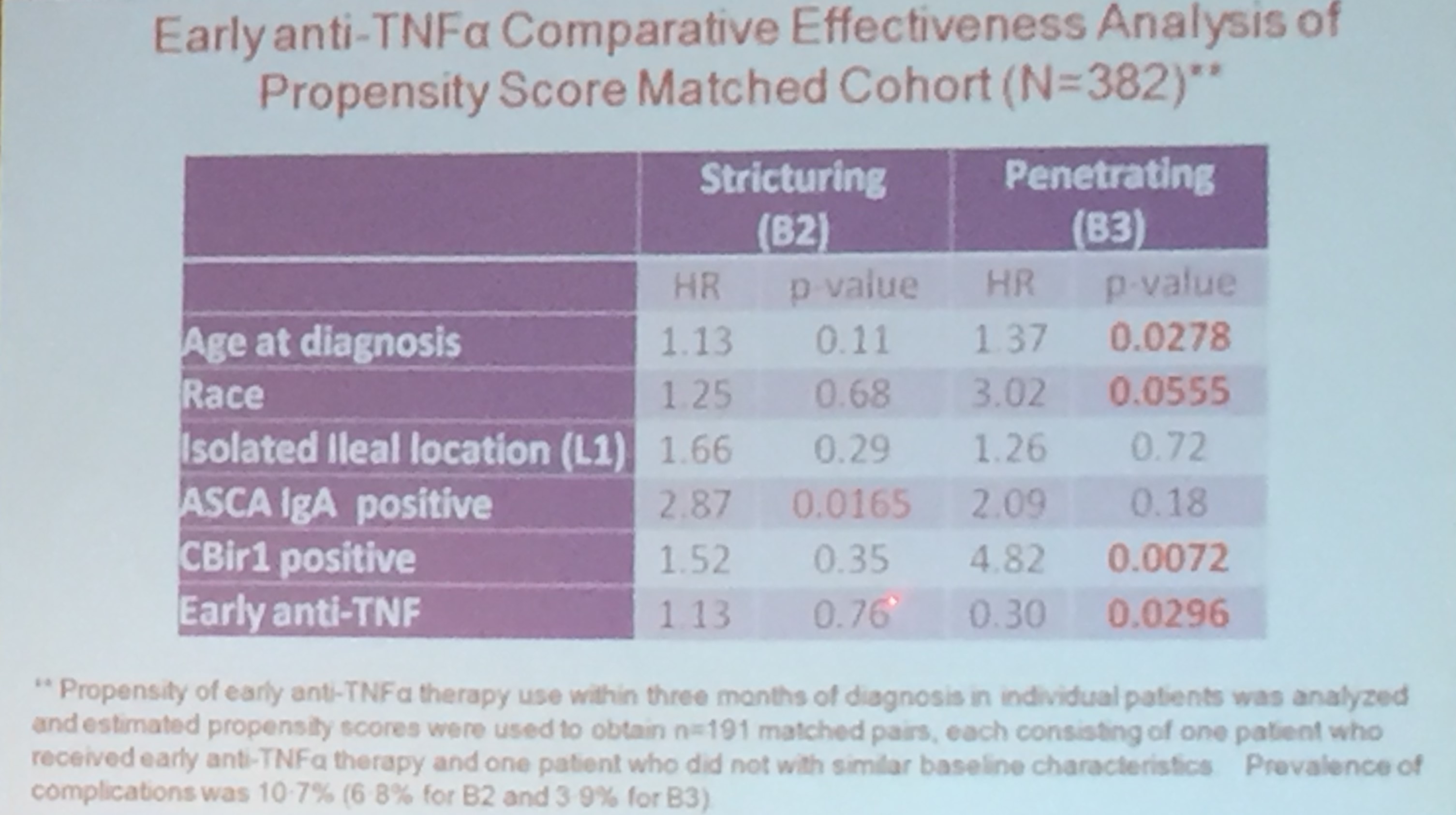
- Early use of biologics (n=145) was associated with slowing of disease progression (hazard ratio 0.85, CI 0.76-0.95). Those who received anti-TNF therapy within three months of diagnosis were less likely to develop stricturing (B2) or penetrating (B3) disease.
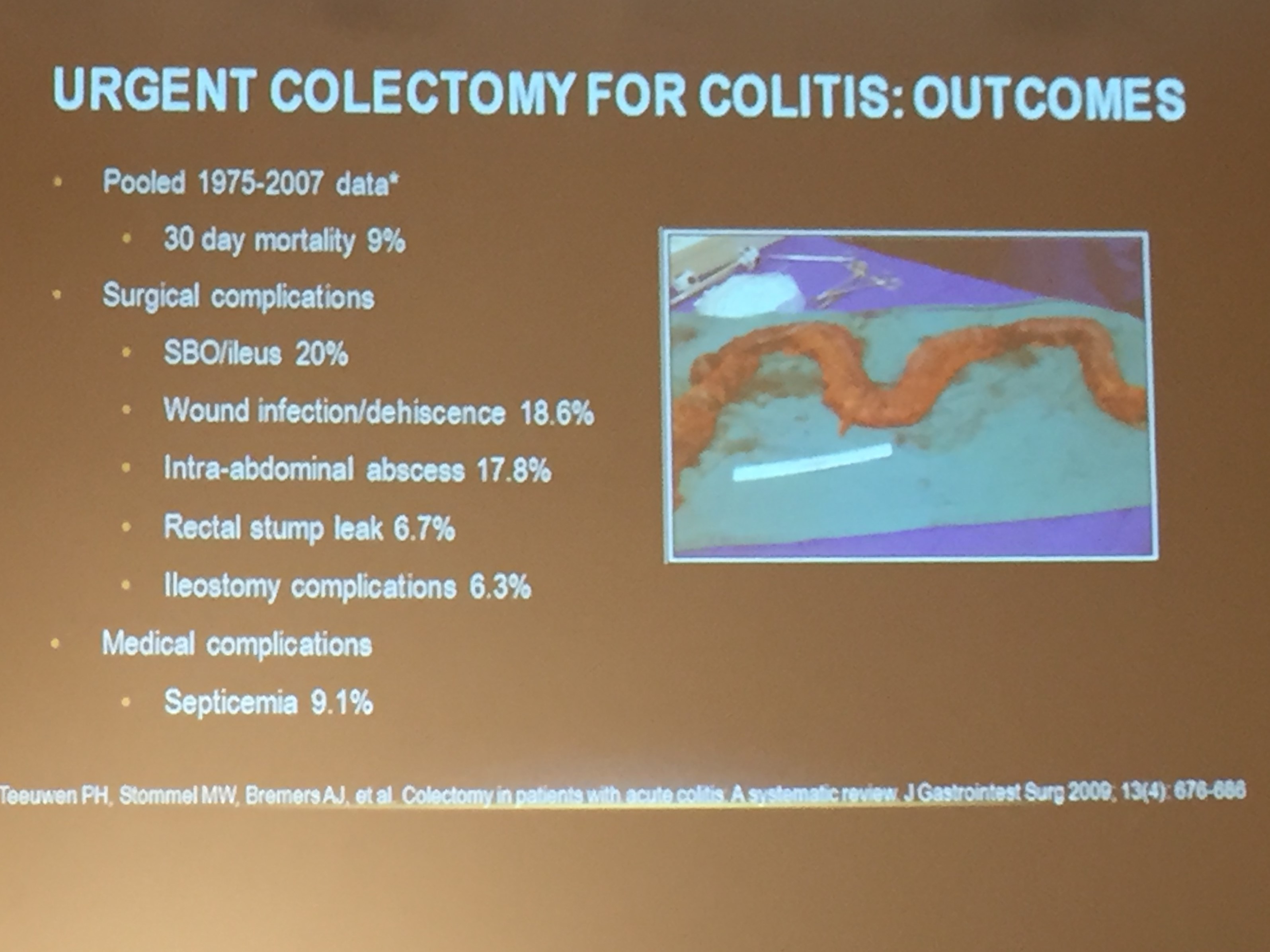
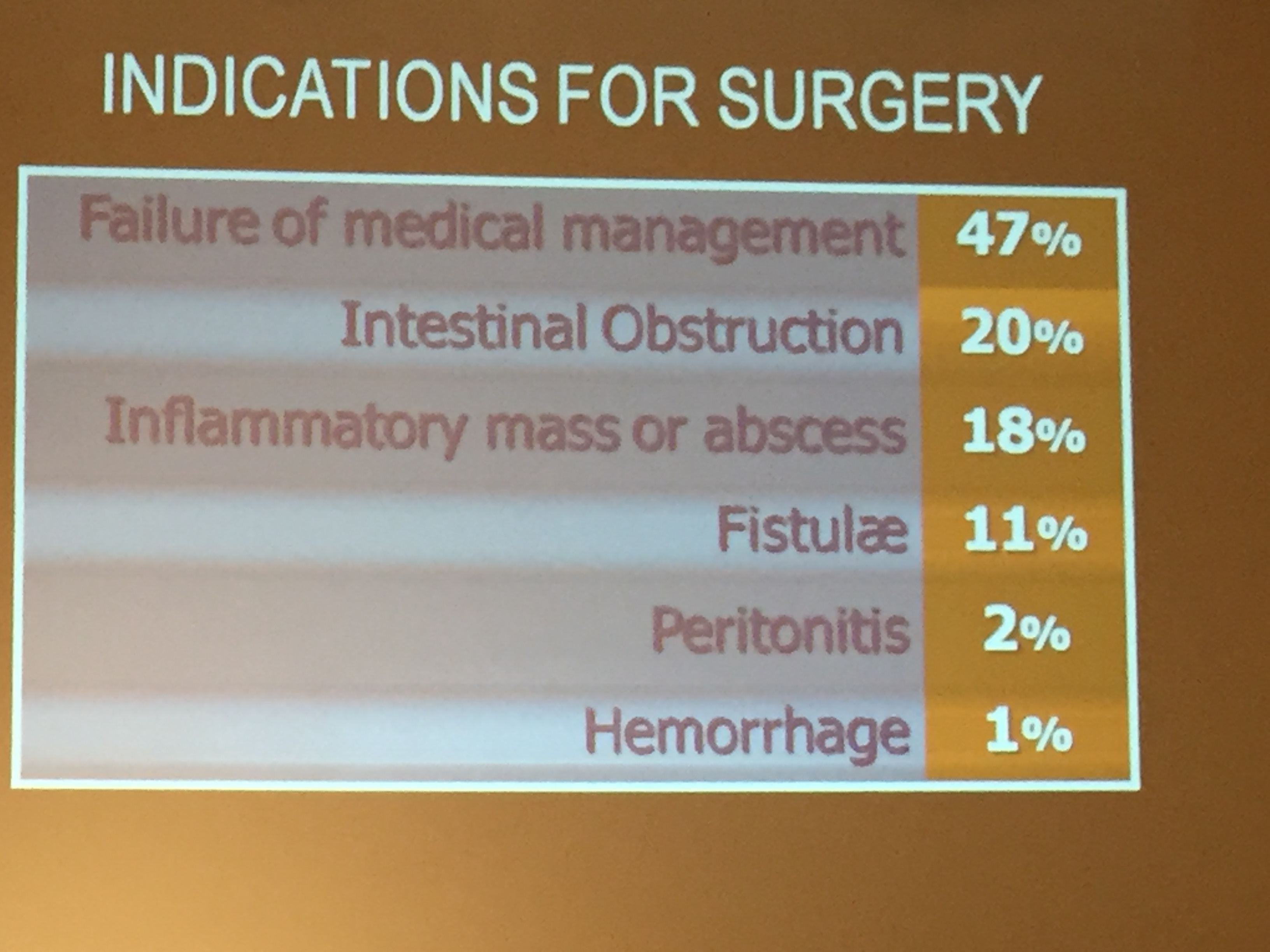
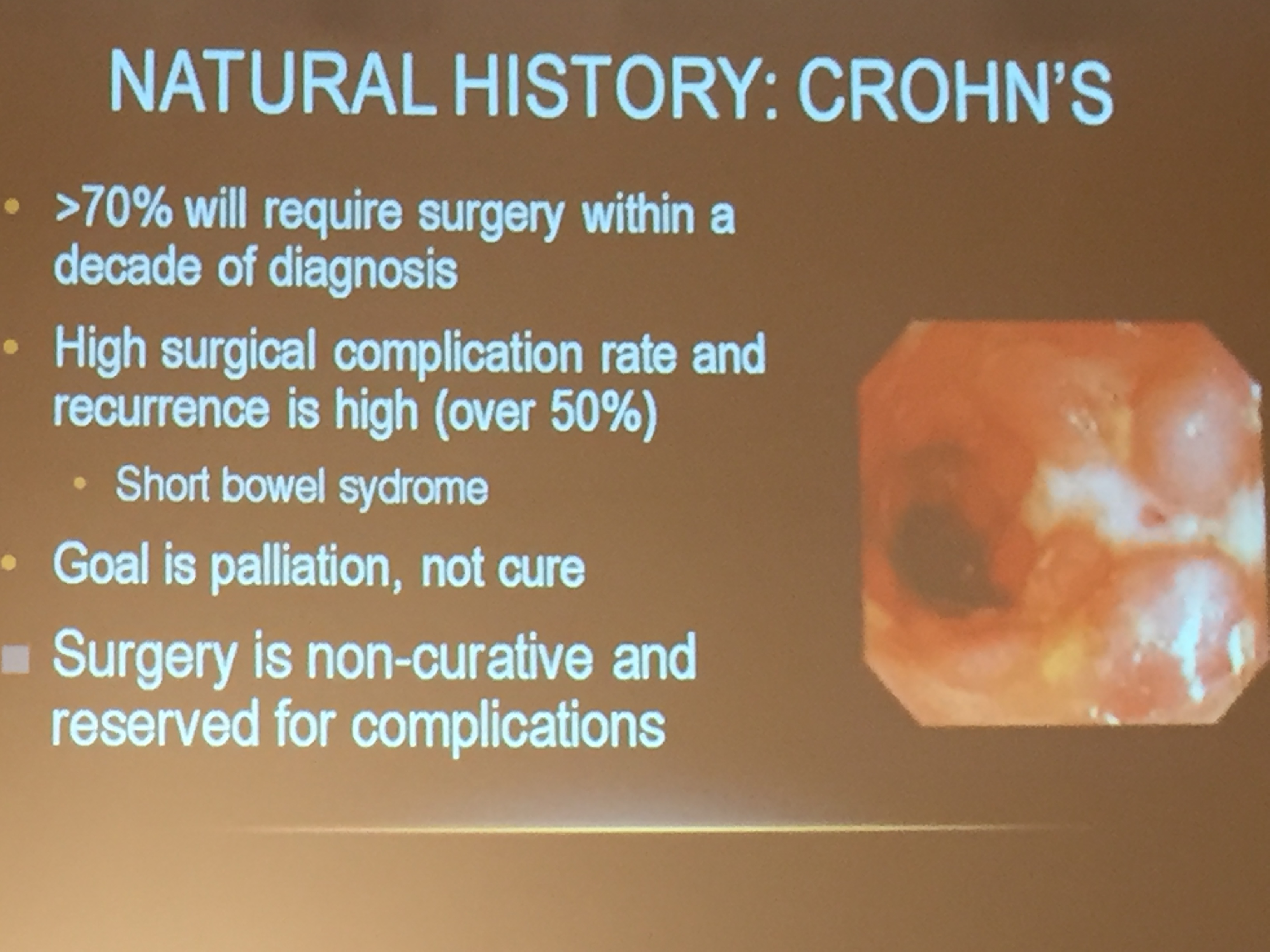
- Early anti-TNF therapy did not effect progression to surgery. Surgery rates were 4% at 1 year, 13% at 5 years, and 26% at 10 years.
- Of those who needed surgery, ~15% already had their first bowel-related surgery in the first 90 days after diagnosis.
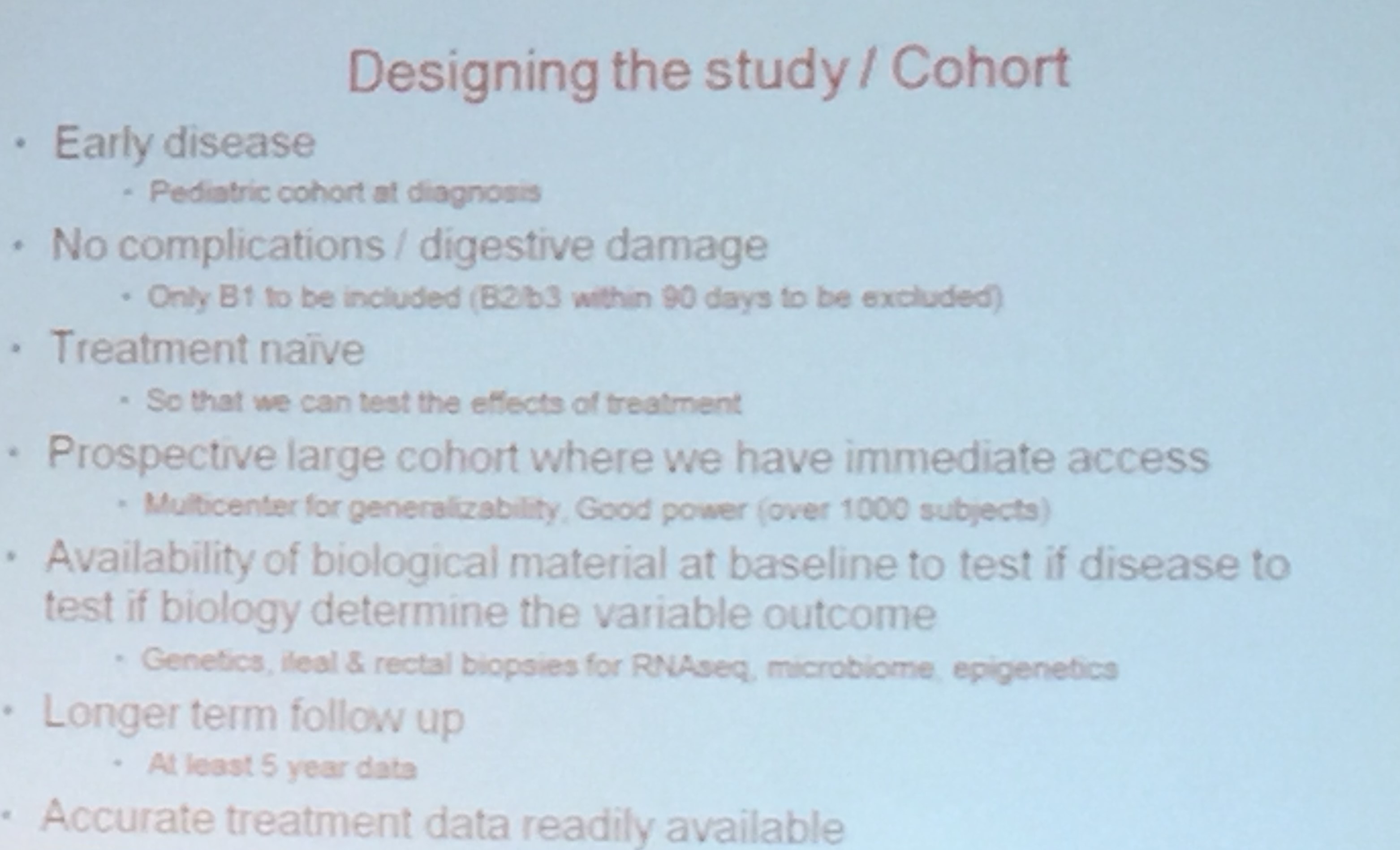
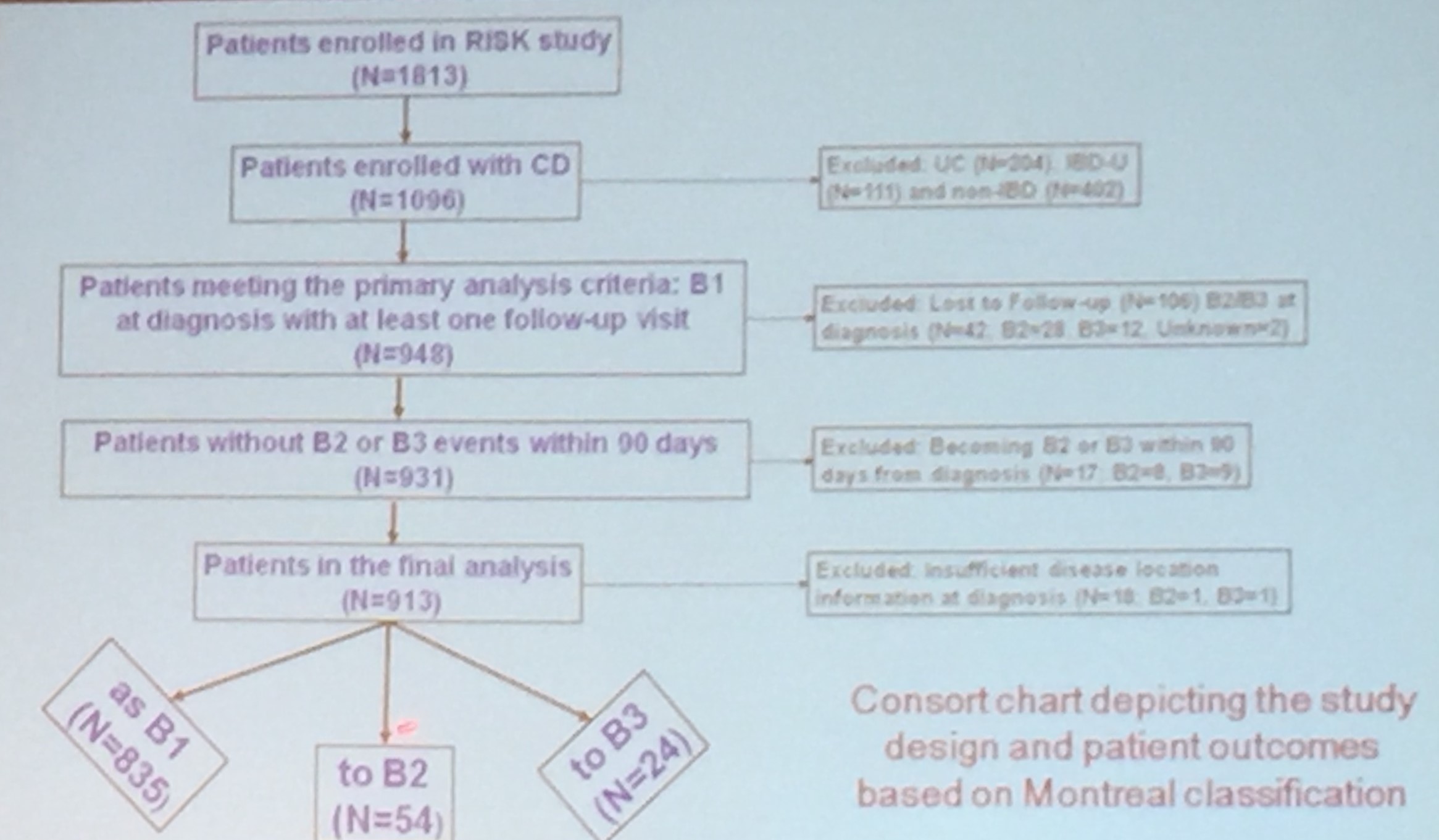
- The study cohort at diagnosis included only 51 with B2 disease, 27 with B3, and 11 with both B2 & B3. Thus, these three disease phenotypes represented ~6% of the entire cohort.
In the editorial, the authors state that this study “is a sobering reminder that we apparently have not changed the long-term course of CD for our pediatric patients.” Though, at the same time, they explain how this study had some limitations which could have affected some of the conclusions.
- In contrast to the RISK study, this study classified patients as B1 who progressed to B2 or B3 in the first 3 months of diagnosis. Including these patients decreased the chance to show improvement with early biologic therapy.
- Also, this cohort included a lower percentage of African American patients compared to the RISK study (8% vs 13%). This also lowered the likelihood of identifying improvement; these patients are more likely to develop penetrating disease which can be prevented with early biologic therapy (RISK study: Kugasthasan S et al. Lancet 2017; 389: 1710-8).
Also, one other finding of the study was that there was a paradoxical increase in the risk of surgery in the first 5 years in the early biologic group. “This suggests that our practicing pediatric gastroenterologists may have selected the sicker patients to start biologics.”
My take: I think biologics do influence the natural history of Crohn’s disease in children. However, this study suggests that the magnitude of that alteration is suboptimal.
Related blog post: CCFA update 2017 -RISK study presentation