
M Joseph et al. JPGN 2025;81:743–747. Duct tales: Biliary anomalies found at endoscopic retrograde cholangiopancreatography in trisomy 21 pediatric patients
Methods: A single-center, retrospective chart review was conducted to identify pediatric patients (n=12) with T21 who underwent ERCP.
Patient characteristics:
- Six patients (50%) had a history of duodenal atresia with subsequent surgical repair during the neonatal period
- Four patients (33.3%) had chronic or acute recurrent pancreatitis, and two patients (16.7%) had biliary pancreatitis
- Five patients (41.7%) had a biliary stricture that required stenting
- Choledocholithiasis was present in 7 of the 12 patients (58.3%)
Key findings:
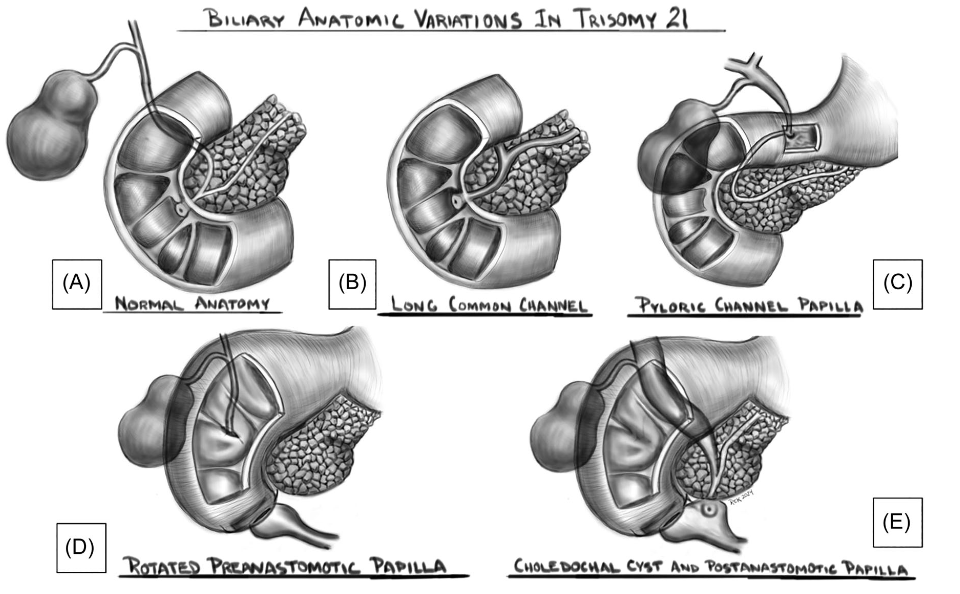
- Eight patients (66.7%) were found to have an abnormal location of the major papilla. This included three patients’ papillae which were in the blind duodenal pouch created after duodenal atresia surgery (Figure 1B) and two patients had their papilla in the proximal duodenum/bulb (Figure 1D)
- Two patients (16.7%) had unsuccessful ERCP either due to difficult cannulation or inability to find the major papilla
My take: In patients with trisomy 21, ERCP may be quite challenging due to anatomic variations and stricturing. In some patients in this cohort, a front-viewing scope was helpful.

