GR D’Haens et al. Gastroenterol 2022; DOI:https://doi.org/10.1053/j.gastro.2022.01.044. Open Access: Higher vs Standard Adalimumab Induction Dosing Regimens and Two Maintenance Strategies: Randomized SERENE CD Trial Results
Methods: In this phase 3, randomized, double-blind, multicenter trial, eligible adults were randomized to higher induction regimen (adalimumab 160 mg at weeks 0, 1, 2, and 3; n = 308) or standard induction regimen (adalimumab 160 mg at week 0 and 80 mg at week 2; n = 206) followed by 40 mg every other week from week 4 onward. Endoscopic results were interpreted by a central reviewer.
Key Findings:
- Similar proportions of patients receiving higher induction regimen and standard induction regimen achieved clinical remission at week 4 (44% in both; P = .939) and endoscopic response at week 12 (43% vs 39%, respectively, P = .462).
- There was a high proportion of patients (>70%) who achieved corticosteroid-free clinical remission after an early corticosteroid taper beginning at week 4
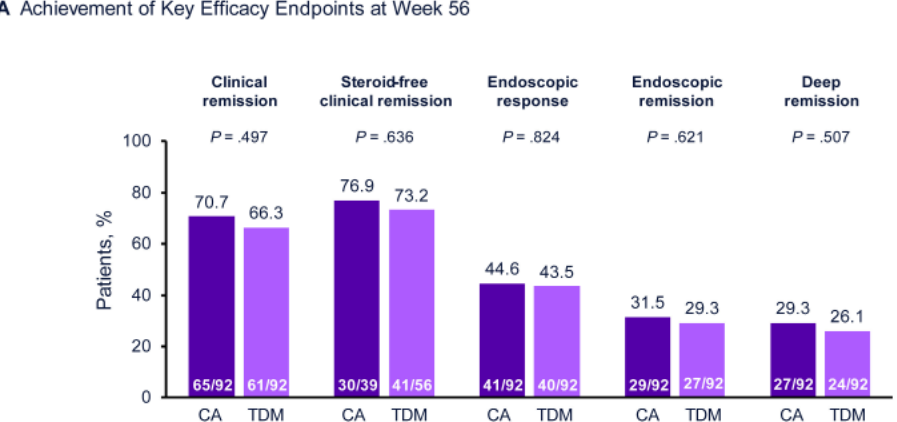
- Week 56 efficacy was similar between clinically-adjusted (CA) and therapeutic drug monitoring (TDM). 28% of patients in the CA group and 39% of TDM had their dose escalated.
- Safety profiles were comparable between dosing regimens.
In the discussion, the authors wade into the topic of TDM for adalimumab:
“Results from the exploratory SERENE CD study suggesting there is no clinical benefit of a proactive TDM strategy over a CA strategy for optimizing adalimumab maintenance dosing align with the results from previous studies evaluating TDM of anti–tumor necrosis factor therapies in adult patients with inflammatory bowel disease. In the TAXIT study, proactive TDM was not superior to CA dose optimization for achieving remission at 1 year in patients with CD or ulcerative colitis.24 Similarly, in the TAILORIX study of patients with CD, proactive TDM failed to improve clinical and endoscopic remission rates over a CA approach.25 In contrast, proactive TDM led to a higher clinical remission rate than did reactive TDM among pediatric patients with CD in the PAILOT trial, but this trial was nonblinded and lacked endoscopic assessments.26“
My take: This study shows that standard induction performed as well as higher dose induction in adults with Crohn’s disease. Also, this study found that TDM did not improve response at 56 weeks in adults. Due to differences in body size and metabolism, the exact role for TDM in pediatric patients needs further study.
Related blog posts:
- Low Anti-TNF Levels or Antibodies Are Associated with Antibodies to Subsequent Anti-TNF Agent
- Better Levels –>Better Outcomes with Adalimumab
- “Do Not Stop Anti-TNF Medications in Children with IBD When They Are Working”
- What about Combination Therapy with Adalimumab?
- Vedolizumab vs Adalimumab: Histology Outcomes from Varsity Trial
- Ustekinumab vs Adalimumab: Head-to-Head Study
- Updated Adalimumab Dosing and Ustekinumab for Refractory Pediatric UC
- For Next Insurance Appeal: TDM for Adalimumab & Satire on PA
- Here’s the Proof That Proactive Therapeutic Drug Monitoring Improves Outcomes in Children with Crohn’s Disease
- Immune-Mediated Reactions to Anti-TNFs and What to Do About Them