These videos are on TikTok account. I do not have an account but was able to access this short video on my laptop (had trouble accessing on my mobile):
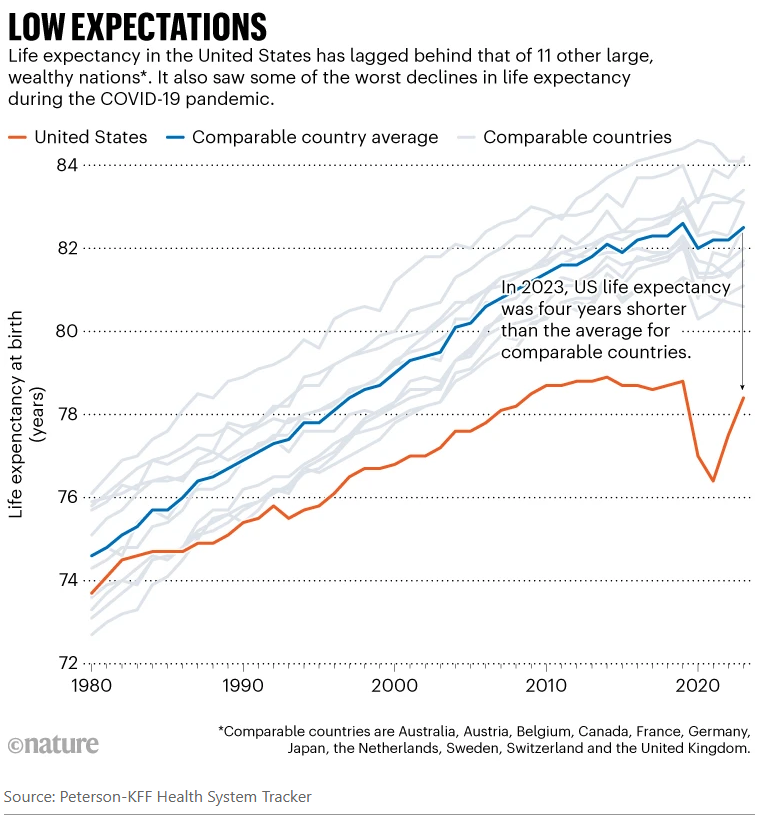
Since taking over as the top US health official in February, Robert F. Kennedy Jr has overseen radical changes that have alarmed many public-health experts…His mission, he says, is to ‘Make America Healthy Again’. “We are the sickest nation in the world,” he said in March, “and we have the highest rate of chronic disease.” His diagnosis holds some truth, say public-health specialists and analysts. Relative to other similarly wealthy nations, the United States has the shortest life expectancy despite spending the most on health care…And researchers agree that high rates of chronic disease, including heart disease and obesity, are key contributors to Americans’ higher death rates, as Kennedy emphasizes.
But researchers say that Kennedy — widely known as RFK Jr — has mostly ignored other leading causes of death and ill health, including car accidents, drug overdoses and gun violence…
Life expectancy in the United States was closer to the average for its peers around 1980 and gradually improved, according to KFF’s analyses. The gains were driven partly by a drop in smoking and increased use of cholesterol-lowering drugs known as statins…
Overall, chronic conditions — heart disease, cancer, stroke and respiratory disease — take up four out of five spots on the country’s list of biggest killers…One of the biggest drivers of those deadly conditions is obesity, say researchers. As of 2022, about 42% of adults were considered obese in the United States, compared with 27% in the United Kingdom and 5.5% in Japan. Obesity increases the risks of developing diabetes, heart disease, cancer and many other conditions. “The US has, particularly around diet, obesity and overweight, adopted unhealthier lifestyles at a higher rate than our country peers,” Bollyky says…
The problems caused by chronic disease are compounded by poor health care. Compared with a group of similar high-income countries, the United States is the only one that lacks universal health-insurance coverage… Lack of health insurance, high costs and other barriers prevent people from getting diagnoses and treatment early on…
The other big contributors to lower life expectancy in the United States — and what really sets the country apart, researchers say — are high death rates from substance misuse, car accidents, suicide and homicide (see ‘Varied causes’). These tend to kill people of working age…All told, the death rates in working-age people mean that one 5-year-old out of every 20 — or roughly one in every school class — will die before the age of 45, according to Angus’s calculations. The comparable figure is one in 50 in the United Kingdom and one in 100 in Switzerland…
Health spending in the United States was about US$13,000 per person in 2023, according to a KFF analysis. That compares to an average of about $7,000 per person in similar large, well-off countries…
Boosting rather than cutting spending on disease prevention is “where the big gains are to be made on population health” [Reginald Williams, a health-policy specialist at the Commonwealth Fund says his] first priority would be to expand health coverage. In the United States, around 8% of people lack health insurance, compared with around 1% or less in similar high-income countries. The second, he says, would be to invest more in primary care — the physicians and other health professionals who are the first port of call for patients, and who deal with disease prevention and management…
Tackling the high death rates from overdoses and guns, meanwhile, would involve addressing entrenched social and political issues such as gun ownership, poverty, unemployment and inequality.
My take: Despite big promises from politicians, there are no quick fixes for improving our national health. Improving health care access would help but this does not address deaths due to firearms, drug overdoses and to car accidents.
Earlier this year, as President Donald Trump was beginning to reshape the American government, Michael, an emergency room doctor who was born, raised, and trained in the United States, packed up his family and left the country…”Part of being a physician is being kind to people who are in their weakest place,” Michael said. “And I feel like our country is devolving to really step on people who are weak and vulnerable…”
The Medical Council of Canada said in an email statement that the number of American doctors creating accounts on physiciansapply.ca, which is “typically the first step” to being licensed in Canada, has increased more than 750% over the past seven months compared with the same time period last year — from 71 applicants to 615. Separately, medical licensing organizations in Canada’s most populous provinces reported a rise in Americans either applying for or receiving Canadian licenses, with at least some doctors disclosing they were moving specifically because of Trump…
While it was once more difficult for American doctors to practice in Canada due to discrepancies in medical education standards, Canadian provinces have relaxed some licensing regulations in recent years, and some are expediting licensing for U.S.-trained physicians…
Michael, the physician who moved to Canada this year, said he had long been wary of what he describes as escalating right-wing political rhetoric and unchecked gun violence in the United States, the latter of which he witnessed firsthand during a decade working in American emergency rooms…
This desire to leave has also been striking to Hippocratic Adventures, a small business that helps American doctors practice medicine in other countries…
Alison Carleton, a family medicine doctor who moved from Iowa to Manitoba in 2017, said she left to escape the daily grind of America’s for-profit health care system and because she was appalled that Trump was elected the first time.Carleton said she now runs a small-town clinic with low stress, less paperwork, and no fear of burying her patients in medical debt.
My take: There are more than one million physicians in the U.S. per AAMC data; so the absolute numbers leaving are quite small. However, this uptick in physicians leaving is another indicator of U.S. physicians being unhappy with U.S. healthcare policy and the direction in which it is headed.
Throughout the United States, PCPs have been leaving traditional practices for concierge and direct primary care (DPC) practices, in which patients are offered personalized and more accessible primary care in exchange for membership or retainer fees… these models can offer physicians notable advantages over traditional primary care models, including greater clinical autonomy, more take-home pay, and improved work–life balance and job satisfaction.4,5 Less burdened by prior authorizations, insurance denials, billing and coding tasks, and other demands in traditional practices — including the need to adhere to regulatory requirements under alternative payment models — physicians often have more time for direct patient care...Yet trade-offs — in the form of decreased access for patients [without a concierge physician] and increased strain on PCPs in traditional primary care — are borne by the rest of society.
RSV, or respiratory syncytial (sin-SISH-uhl) virus, is the leading cause of hospitalization for infants in the US. An estimated 58,000–80,000 children younger than 5 years old are hospitalized each year. Newborns—babies between 0 and 2 months—are the most at risk of being hospitalized with RSV…
But the 2024–2025 season was different—there were two new ways to protect against the infection. One is a maternal vaccine, Pfizer’s Abrysvo, which is given to pregnant people when their third trimester aligns with RSV season (generally September through January)…the other new protection against RSV is a long-acting monoclonal antibody treatment, nirsevimab, which is given to babies under 8 months old as they enter or are born into their first RSV season and may not be protected by maternal antibodies.
For the new study, CDC researchers looked at RSV hospitalization rates across two different RSV surveillance networks of hospitals and medical centers (called RSV-NET and NVSN)…
The analysis found that among newborns (0–2 months), RSV hospitalizations fell 52 percent in RSV-NET and 45 percent in NVSN compared with the rates from the 2018–2020 period.However, when the researcher excluded data from NVSN’s surveillance site in Houston—where the 2024–2035 RSV season started before the vaccine and treatment were rolled out—there was a 71 percent decline in hospitalizations in NVSN.
For a broader group of infants—0 to 7 months old—RSV-NET showed a 43 percent drop in hospitalizations in the 2024–2025 RSV season, and NVSN saw a 28 percent drop.Again, when Houston was excluded from the NVSN data, there was a 56 percent drop.
Lastly, the researchers looked at hospitalization rates for toddlers and children up to 5 years old, who wouldn’t have been protected by the new products. There, they saw RSV hospitalization rates were actually higher in the 2024–2025 season than in the pre-pandemic years.
The United States will withdraw its financial support of Gavi, the global organization that helps purchase vaccines for children in poor countries, Robert F. Kennedy Jr., the United States secretary of Health and Human Services, told the group’s leaders on Wednesday, accusing them of having “ignored the science” in immunizing children around the world…
“Any decision made by Gavi with regards to its vaccine portfolio is made in alignment with recommendations by the World Health Organization’s Strategic Advisory Group of Experts on Immunization (SAGE), a group of independent experts that reviews all available data through a rigorous, transparent and independent process,” Gavi’s statement said…
Dr. Atul Gawande, a surgeon who led global health work in the Biden administration, called Mr. Kennedy’s remarks “stunning and calamitous…”
The United States was the largest donor to Gavi, whose work is estimated to have saved the lives of 17 million children around the world over the past two decades…
Gavi had hoped to raise $9 billion for the 2026-30 period, funds the organization said would allow it to purchase 500 million childhood vaccinations and to save at least eight million lives by 2030. ..
The decision to end U.S. support for Gavi — which was included in the rescission package passed by Congress and now being considered by the Senate — leaves the organization with an immense hole in its budget…The Gates Foundation is maintaining its funding at a stable level from previous years — about $350 million in each of the next four years — as is the United Kingdom.
My take: It is no exaggeration to say that the shift in U.S. vaccine policy may result in hundreds of thousands of deaths every year. In addition, U.S. travelers will be more likely to be exposed to vaccine-preventable illnesses as well.
Health Secretary Robert F. Kennedy Jr. on Monday removed every member of a scientific committee that advises the Centers for Disease Control and Prevention on how to use vaccines and pledged to replace them with his own picks.
Major physicians and public health groups criticized the move to oust all 17 members of the Advisory Committee on Immunization Practices… Kennedy wrote in a Wall Street Journal opinion piece. “A clean sweep is needed to re-establish public confidence in vaccine science…”
Kennedy is going against what he told lawmakers and the public…Kennedy’s move, coupled with declining vaccination rates across the country, will help drive an increase in vaccine-preventable diseases…
Republican Sen. Bill Cassidy of Louisiana, a doctor who had expressed reservations about Kennedy’s nomination but voted to install him as the nation’s health secretary nonetheless, said he had spoken with Kennedy moments after the announcement.
“Of course, now the fear is that the ACIP will be filled up with people who know nothing about vaccines except suspicion,” Cassidy said in a social media post. “I’ve just spoken with Secretary Kennedy, and I’ll continue to talk with him to ensure this is not the case.”
RFK Jr alleges ACIP committee members are laden with conflicts of interest as the rationale for this move; however, his editorial lists little evidence of this. Just last month, HHS leaders announced that COVID vaccination was no longer recommend for pregnant women; these women and their infants in the first 6 months of life are at increased risk of COIVD deaths and complications. The pattern of undermining expertise in utilizing vaccines will have far-reaching repercussions. Unfortunately, the trajectory for public health is even more worrisome. It is likely that there will be more measures to limit vaccine availability. Though, it will be a while until the full body count will be determined.
My take: Senator Cassidy, a physician, allowed RFK Jr to lead HHS despite misgivings; this was due to political considerations rather than qualifications. This decision and his lack of action to hold him accountable are a true betrayal of his constituents and to the principle of ‘Do No Harm.’
It is funny that the city of Roswell highlights an award for excellence in park and recreation management on a trashcan. This type of honor, though, could be replicated for the work of the current HHS secretary.
Yesterday, a ICU colleague indicated that she really does not like to work on summer holiday weekends. While she is a hard worker, what she doesn’t like is seeing kids with drowning and firework injuries. All of a sudden a happy time becomes tragic. With that in mind, here are a few tips to prevent drowning.
Also, firearm deaths are the leading cause of death in children in the U.S. and motor vehicle accidents are second. So, firearms need to be secured and drive safely on the way to the pool, lake, river or beach.
CP Duggan, ZA Bhutta. NEJM 2025; DOI: 10.1056/NEJMp2503243. “Putting America First” — Undermining Health for Populations at Home and Abroad
This article initially lays out the historical context of U.S. involvement in global health dating back to aiding famine in Belgium (1917), WHO (1948), USAID (1961). Also, the CDC and NIH have played important roles following WWII. Subsequently, the commentary outlines the impact of dismantling U.S global health efforts. In the two related articles cited afterwards, it is clear that the cuts to foreign aid and other DOGE activities may result in millions of deaths and at the same time expand the federal deficit.
An excerpt:
In the initial months of the Trump administration, numerous executive orders have led to a chaotic dismantling of U.S. foreign-assistance and global health efforts. These orders have already had, and will continue to have, severe adverse effects on vulnerable populations globally. But they also have serious implications for people in the United States…
Often missing from these success stories are the financial and health-related benefits these programs have had in the United States….One of the earliest and most fundamental examples of reciprocal innovation was the discovery and implementation of oral rehydration therapy (ORT)…Widespread use of ORT has helped drive substantial reductions in childhood deaths from diarrhea and has led to a new standard of care for childhood diarrhea in high-income countries and to commercial products in the United States…
Perhaps no program epitomizes these dual advantages better than the President’s Emergency Plan for AIDS Relief (PEPFAR). Early in the HIV epidemic, the NIH promoted multinational scientific collaborations to identify the virus, develop effective treatments, and implement global prevention and treatment programs, which led to PEPFAR’s creation in 2003. PEPFAR has saved 26 million lives, and economic growth in countries with PEPFAR programs has benefited the United States and other trading partners…[and] have contributed enormously to current knowledge about HIV and AIDS.
Another essential initiative, the FIC — the NIH institute responsible for supporting research training and partnerships in global health — has …directly benefited health in the United States by advancing early cancer detection and the development of sickle cell disease therapies, point-of-care diagnostics for infectious diseases, and treatments for child malnutrition. More than three quarters of FIC grants involve a U.S. grantee or investigator, which further emphasizes the institute’s direct benefits to the U.S. economy…
Since U.S. foreign assistance accounts for about 1% of the federal budget, we are skeptical of cost-savings–based arguments for its elimination…
The Trump administration’s gutting of USAID and other foreign-assistance programs marks a break from decades of evidence-based practices that have improved lives throughout the world. In addition to pushing millions of people into poverty and leading to an estimated 160,000 or more avoidable child deaths each year,4 these reforms will undermine health and the economy in the United States…
Withdrawal from the WHO reduces the United States’ ability to influence reform and restructuring of the world’s global health coordinating body. The elimination of U.S. funding for Gavi, the Vaccine Alliance, also endangers the health of vulnerable populations internationally and in the United States…
Critical to the success of advocacy efforts will be evidence of the ways in which the withdrawal of foreign aid and global disengagement undermine health and economic well-being in the United States and threaten global health and economic security.
My take: By the time the extent of the damage is understood, it will be too late to fix what this administration has destroyed. The toll in terms of death and suffering both in the U.S. and abroad will be hard to justify and not further the aim of making ‘America First.’
Related articles:
D Wallace-Wells, NY Times 5/8/25: The $200 Billion Gamble: Bill Gates’s Plan to Wind Down His Foundation “He is committing the foundation to 20 more years of generous aid, more than $200 billion in total, targeting health and human development…The news comes at a time that will seem to many as a perilous one, given the Trump administration’s recent assault on foreign aid and indeed on the idea of global generosity itself….The journal Nature suggested that an overall cessation of U.S. aid funding could result in roughly 25 million additional deaths over 15 years.”
J Riedl, The Atlantic 5/8/25: The Actual Math Behind DOGE’s Cuts “As an effort to meaningfully reduce federal spending, however, DOGE remains wholly unserious…The DOGE website now claims $165 billion in savings. However, it still details only a fraction of the supposed cuts, and earlier accounting errors have given way to new ones…Even assuming that the website’s stated savings have become twice as accurate as they were in February, annual savings would reach perhaps $15 billion, or 0.2 percent of federal spending…Total federal outlays in February and March were $86 billion (or 7 percent) higher than the levels from the same months a year ago, when adjusted for timing shifts. This spending growth—approximately $500 billion at an annualized rate—continues to be driven by the three-quarters of federal spending allocated to Social Security, Medicare, Medicaid, defense, veterans’ benefits, and interest costs. These massive expenses have been untouched by DOGE’s focus on small but controversial targets such as DEI contracts and Politico subscriptions…The bad news is that the project seems quite likely to expand long-term budget deficits. Slashing IRS enforcement will embolden tax evasion and reduce revenues by hundreds of billions of dollars over the decade. Laying off Department of Education employees who ensure collection of student-loan repayments will increase the deficit. Illegally terminated federal employees are already being reinstated with full back pay, leaving the government with little to show for its trouble besides mounting legal fees…None of this is to say that DOGE has failed. Musk might not have followed through on his unfocused and evolving promises to eliminate payment errors, balance the entire budget, and implement regulatory reform. But he has successfully given the White House cover to purge and intimidate the civil service, helped Congress justify exorbitant tax cuts, rewarded MAGA voters with revenge against their perceived enemies, and granted himself the ability to access sensitive government data and possibly ensure his companies’ continued government contracts. Sure, annual budget deficits remain on track to double over the next decade. But if you thought DOGE was really about cutting costs, you were never in on the joke.”
View of the Chattahoochee River from Don While Memorial Park, Sandy Springs, Ga
Methods: Here we characterize the trajectory by which the gut microbiome recovers its taxonomic and functional profile after antibiotic treatment in mice on regular chow (RC) or Western Diet (WD).
Key findings: “Only mice on RC undergo a rapid successional process of recovery. Metabolic modelling indicates that a RC diet promotes the development of syntrophic cross-feeding interactions, whereas in mice on WD, a dominant taxon monopolizes readily available resources without releasing syntrophic byproducts. Intervention experiments reveal that an appropriate dietary resource environment is both necessary and sufficient for rapid and robust microbiome recovery, whereas microbial transplant is neither.”
Conclusion (from authors): “Our data challenge widespread enthusiasm for faecal microbiota transplant (FMT) as a strategy to address dysbiosis, and demonstrate that specific dietary interventions are, at a minimum, an essential prerequisite for effective FMT, and may afford a safer, more natural and less invasive alternative.”
My take: This study suggests that the best way to get a “healthy” microbiome is to eat a healthy diet rather than to try to alter with FMT. This finding likely would be the same for probiotics as well.
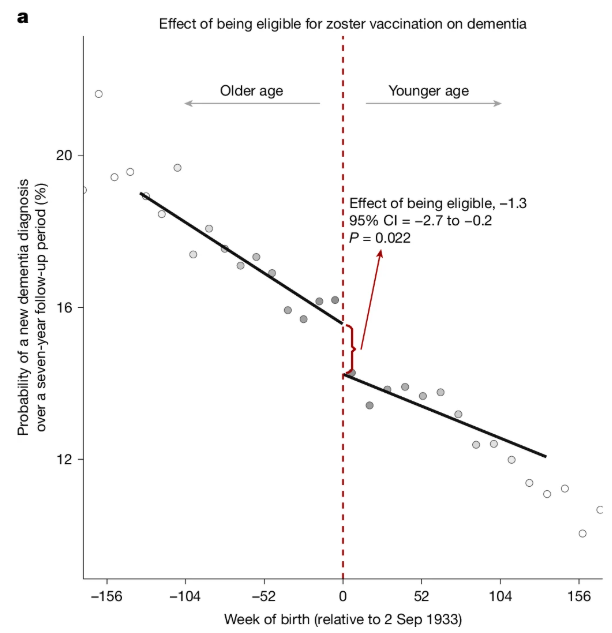
It’s been shown that reactivation of the chickenpox virus can lead to the accumulation of aberrant proteins associated with Alzheimer’s…
The new research, published Wednesday in Nature, analyzed data from more than 280,000 older adults in Wales and found that people who received the original shingles live virus vaccine were 20% less likely to develop dementia of any type than those who were not vaccinated...
The new study was possible because of an unusual public health policy in Wales that provided a “natural experiment” to explore the potential impact of the vaccine on dementia risk. With the rollout of the vaccine on Sept. 1, 2013, in Wales, shots were offered to people who were 79 on that date but not given to people who had turned 80.That allowed the German and Stanford University researchers to compare two groups of people with similar health characteristics who differed only by one week in age...
Bolstering the case for the shingles vaccine protecting against dementia were the findings from a study published in Nature Medicine in 2024 that analyzed medical records from more than 100,000 patients. That analysis suggested the newer shingles vaccine was associated with even better protection against dementia.