
Category Archives: General Health
The Indispensable Physician
A recent pair of commentaries (RM Wachter, L Goldman. NEJM 2016; 375: 1009-1011, R Gunderman. NEJM 2016; 375; 1011-13) provides some insight into what has been gained and what has been lost with the proliferation of hospitalist care in the past 20 years.
The growth of hospitalist care has developed due to numerous factors:
- evidence of cost savings/better outcomes
- need for rapid evaluation of acutely ill patients/repeated evaluations which would be disruptive to efficient outpatient physician practices
Decline of comprehensive care:
- at times of extreme vulnerability when admitted to the hospital, patients have a physician assigned to them who they have probably never met. This has led to a diminishment of the patient-physician relationship.
- increasing number of physicians creates opportunities for miscommunication, particularly on admission and discharge, but also at every step of hospital care during “handoffs”
The second commentary, in particular, challenges the way medicine is evolving. This article stresses the central role of the physician as opposed to the hospital filling that role.
“The reality is that medicine can be practiced without hospitals, but hospitals cannot function without physicians.”
The goal of developing personal relationships with our patients is often at odds with work-life balance. Thus, having hospitalists and other ways of having cross-coverage, when we are unavailable, often conflict with being able to provide the best care.
My take (from 2nd commentary): “The true core of good medicine is not an institution but a relationship — a relationship between two human beings.”
Related blog posts:
- “Weekend Effect” –From the Other Side of the Bed | gutsandgrowth Are hospitals really Focused on patients or their physicians/employees?
- “I’ve Got the Best Doctor” | gutsandgrowth
- Better Discharge Planning Needed | gutsandgrowth
- Increasing Rates of Professional Burnout | gutsandgrowth
- “It is never boring to be a physician” | gutsandgrowth

Glacier Nat’l Park
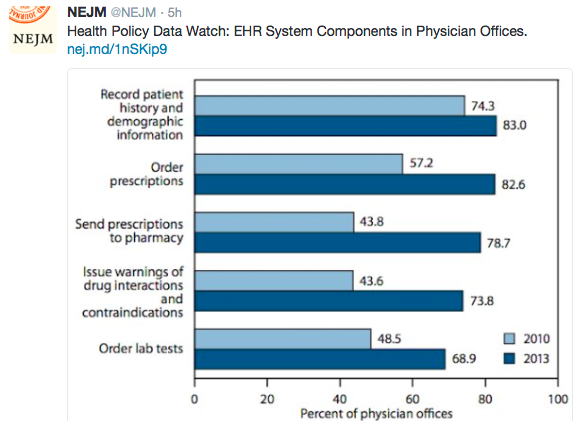
Image Only: Suicide Rates by Age Groups
Image

Image Only -Mortality from Cancer and Heart Attacks
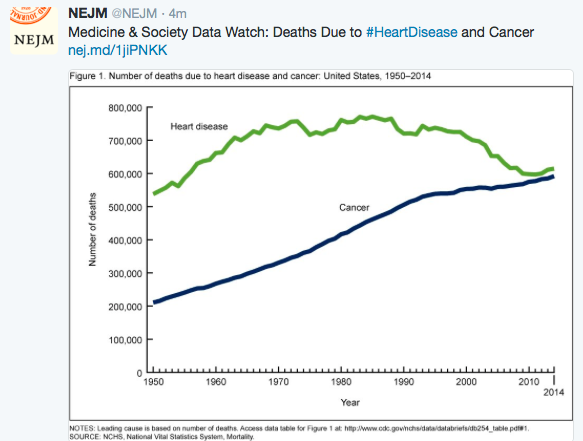
Image Only -Change in Teen Pregnancy Rates

Related blog post:
Is a Gluten-Free Diet a Healthy Diet for Those without Celiac Disease?
A helpful commentary (NR Reilly. J Pediatr 2016; 175: 206-10) on the gluten-free diet (GFD) tries to separate fact from fiction. A few key points:
- There are some health problems that can occur with a GFD, particularly when the diet is started without the support of an experienced dietician. GFD foods frequently contain a greater density of fat and sugar and can contribute to obesity and metabolic syndrome. A GFD may lead to nutrient deficiencies in B vitamins, folate, and iron. GFD without sufficient dietary diversity may contain increase in toxin exposures (eg. arsenic, and mercury).
- Gluten is not toxic. “There are no data to support the theory of an intrinsically toxic property of gluten for otherwise-healthy and asymptomatic adults and children, and certain studies have specifically demonstrated a lack of toxic effects.“
- Most individuals with NonCeliac Gluten Sensitivity (NCGS) do not have NCGS! First of all, many receive a GFD without proper testing to exclude celiac disease. Secondly, most will tolerate gluten reintroduction. In an Italian study, “only 6.6% of consecutive patients with presumed gluten sensitivity…actually had NCGS. 86% did not experience symptoms when gluten was reintroduced.”
- Timing of gluten introduction: “The most current understanding…in at-risk infants is that neither delaying gluten introduction from the recommended 6 months of age to 1 year, nor introducing at 4 months of age alters long-term CD risk estimates.”
My take: This is an excellent commentary. While many people (without celiac disease) perceive benefit from a GFD, only a minority are likely to derive better health or improved quality of life. Those who stick with a GFD should seek the help of a well-qualified dietician.
Related blog posts:
- An Unexpected Twist for “Gluten Sensitivity” | gutsandgrowth
- The Science Behind IBS Dietary Interventions | gutsandgrowth
- Gluten sensitivity without celiac disease | gutsandgrowth
- Food choices, FODMAPs, and gluten haters | gutsandgrowth

Glacier Nat’l Park
Medical Error -Overestimated as Cause of Death
A recent NY Times article provides some context to previous studies claiming that medical error could cause 100,000-250,000 deaths per year: Aaron Carroll Death by Medical Error
Here’s some excerpts:
When I started out as a doctor in 1999, the Institute of Medicine published a blockbuster report that declared that up to 98,000 people were dying in United States hospitals each year as a result of preventable medical errors. Just a few months ago, a study in the BMJ declared that number has now risen to more than 250,000, making preventable medical errors in hospitals the third-largest cause of death in the country in 2013…
There are about 2.5 million deaths each year in the United States, about 700,000 of which are hospitalized patients. This means that medical errors — in hospitals — would have to account for up to 10 percent of all deaths, or up to more than a third of hospitalized patients. That’s hard to fathom….
It’s somewhat sensationalistic to keep coming up with increasing numbers. I’m not sure it’s doing much good. After the publication of the initial report, defenders of the 98,000 number argued that even if the numbers were wrong, bringing attention to this problem would be good in itself.
Unfortunately, research doesn’t necessarily back that up. A 2010 study in The New England Journal of Medicine followed 10 North Carolina hospitals in the 10 years after the Institute of Medicine report. They found that the overall rate of harms, and the rate of preventable harms, did not significantly improve over that period.
My take: The article, in full, makes some compelling arguments that medical errors are overly-attributed as causes of death. At the same time, the article does not dismiss the importance of medical errors. Many of the harms from medical errors do not result in death.

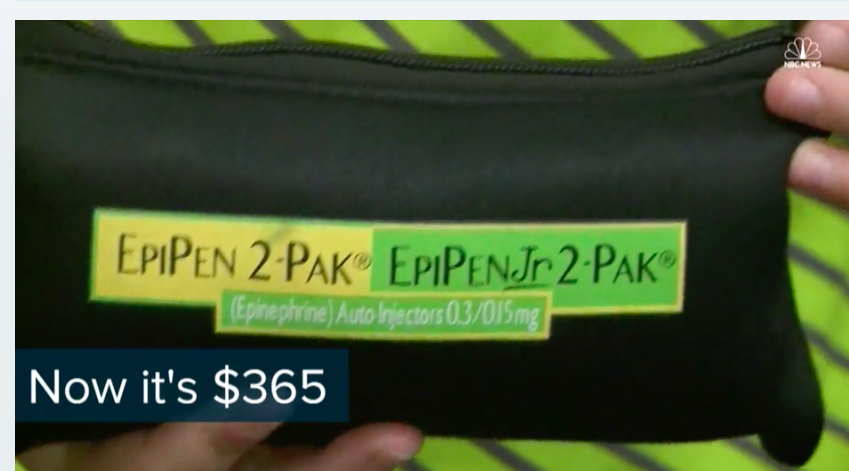
Another Day, Another Exorbitant Drug Increase for a Vital Drug: Epipen
From NBC News: EpiPen Prices Rocket Along With Drugmaker Executive’s Pay
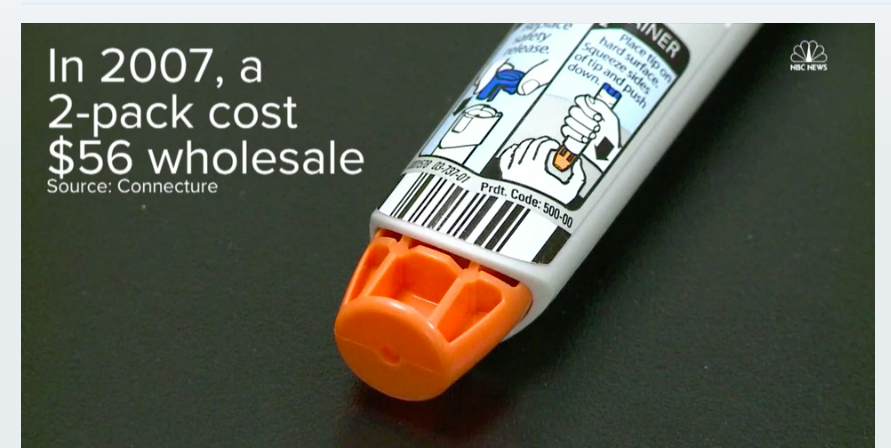

Also, this story has been discussed in NY Times (Epipen & Health Care System Dysfucntion) and USA Today (see below)

Also, from KT Park’s twitter feed:

Petaloid Cataract
“The petaloid cataract is classically seen in patients who have had blunt trauma to the eye.” NEJM: Petaloid Cataract

Raynaud’s Phenomenon
IN 1862, Maurice Raynaud described a 26-year-old female patient: “Under the influence of a very moderate cold…she sees her fingers become ex-sanguine, completely insensible, and of a whitish-yellow color. This phenomenon …lasts a variable time, and terminates by a period of very painful reaction, during which the circulation is re-established…and recurs to the normal state.”
An updated review on Raynaud’s: FM Wigley, NA Flavahan. NEJM 2016; 375: 556-65.
This review highlights treatments and the differential diagnosis of primary Raynaud’s phenomenon form secondary causes (eg scleroderma, SLE, dermatomyositis, Sjogren’s and others).

A) Pallor phase B) Cyanotic phase C) Normal nailfold capillaries (primary phenomenon) D) Abnormal nailfold capillaries typical of microvascular disease
