For those of you with an interest in improving our healthcare system, I highly recommend either Eric Topol’s Ground Truths Podcast with Mark Cuban or the transcription of their discussion. Both can be found here: Mark Cuban: A Master Disrupter for American Healthcare
Mark Cuban describes the expansion of his generic pharmacy business Cost Plus Drugs. But the main focus is on other aspects of healthcare like pharmacy benefits managers, insurance companies and improving patient access.
“So a big part of my time these days is going to CEOs and sitting with them and explaining to them that you’re getting ripped off on both your pharmacy and your healthcare side….”
“Because when you see stories like we’ve all seen in news of a big healthcare, a BUCA healthcare (Blue Cross Blue Shield (BCBS), UnitedHealth, Cigna, and Aetna/CVS) plan with all the pre-authorizations and denials, typically they’re not even taking the insurance risk. They’re acting as the TPA (third party administrator) as the claims processor effectively for whoever hired them. And it goes back again, just like I talked about before. And as long as CMS hires or allows or accepts these BUCAs with these plans for Medicare for the ACA (Affordable care Act), whatever it may be, it’s not going to work. As long as self-insured employers and the 50 million lives they cover hire these BUCAs to act as the TPAs, not as insurance companies and give them leeway on what to approve and what to authorize and what not to authorize. The system’s going to be a mess, and that’s where we are today.”
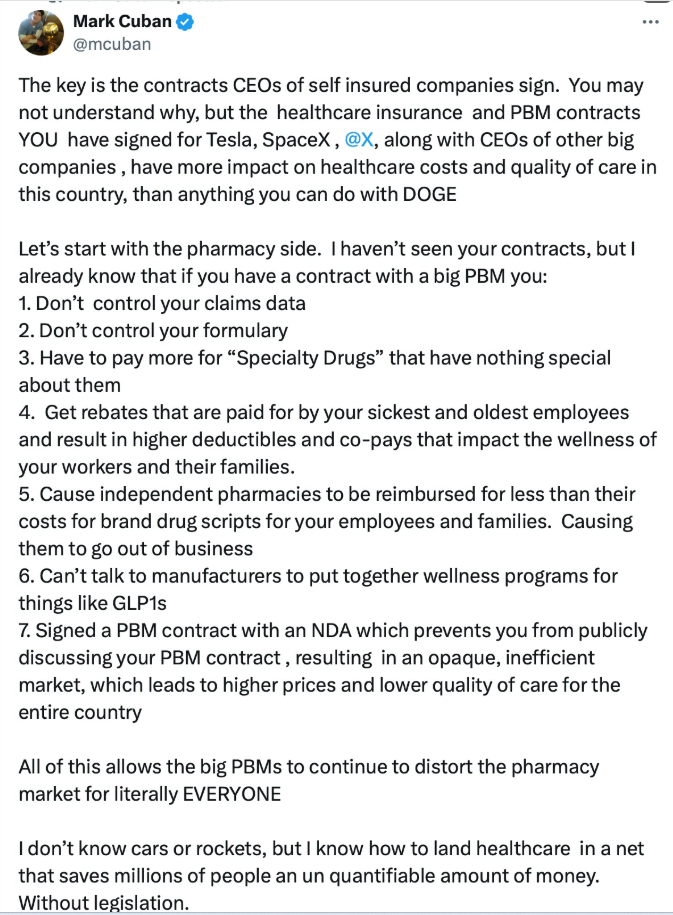
In response to a post by Elon Musk that Americans are not getting a good deal with their healthcare expenditures, Mark Cuban posted the following:
“Because we’re cutting out all those ancillary costs and credit risk, I want Medicare pricing. Now the initial response is, well, Medicare prices, that’s awful. We can’t do it. Well, when you really think about the cost and operating costs of a hospital, it’s not the doctors, it’s not the facilities, it’s all the administration that cost all the money. It’s all the credit risks that cost all the money. And so, if you remove that credit risk and all the administration, all those people, all that real estate, all those benefits and overhead associated with them, now all of a sudden selling at a Medicare price for that hip replacement is really profitable.”
He also describes how his employees pay premiums but no additional costs and how to get to universal health coverage. “Why do we need insurance companies if they’re not even truly acting as insurance companies?“
Related blog posts: