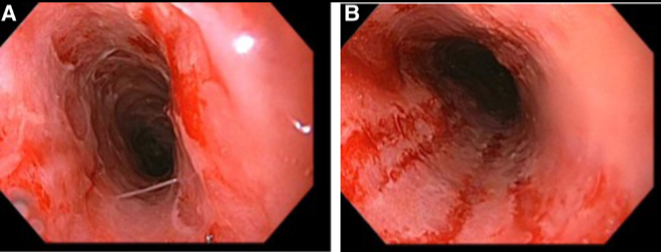
This case report describes a 17 yo with sore throat, odynophagia chest pain, and dysphagia associated with vaping. His symptoms resulted in hospitalization and he underwent an EGD on day 4 after symptoms had not improved with multiple empiric therapies.
EGD findings included .
Circumferential erosive or exudative lesions) esophagitis with bleeding found throughout the entire esophagus. Given the lack of infectious etiologies, the authors made a diagnosis of vaping-associated esophagitis
H pylori gastritis
My take: When adolescent patients present with esophageal symptoms, inquiring about exposure to vaping along with medications known to cause pill-esophagitis, is worthwhile.
Methods: The authors in this study developed a 7-point medical complexity score . One point was assigned for each comorbid diagnosis in the following categories: airway anomaly, neurologic, cardiac, respiratory, gastrointestinal, genetic diagnoses, and prematurity. A retrospective chart review was conducted of patients (n=234) seen in the aerodigestive clinic who had ≥2 visits between 2017 and 2021.
Improvements were followed in the Functional Oral Intake Scale (FOIS)–assigned by aerodigestive feeding therapists.6 The FOIS scale is as follows:
•1 = Nothing by mouth
•2 = Tube-dependent with minimal attempts of food or liquids (<10%)
•3 = Tube-dependent with consistent oral intake of food or liquids
•4 = Total oral diet of a single consistency
•5 = Total oral diet with multiple consistencies, but requiring special preparations or compensations
•6 = Total oral diet with multiple consistencies without special preparation, but with specific food limitations
•7 = Total oral diet with no restriction, or <12 months of age on age-appropriate diet
Key findings:
At presentation, 69.5% were not at unrestricted age-appropriate diet; 22.7% of the cohort (n = 53) were completely tube dependent
There were 165 patients who were not at unrestricted total age-appropriate oral diet at presentation, and the majority (54% [n = 90]) showed improvement in their FOIS scores after aerodigestive team intervention.
“For each 1-unit increase in complexity score, there was a 33% decrease in the odds of improvement in FOIS scores (OR, 0.66; 95% CI, 0.51-0.84; P = .001);” however, only neurological comorbidity (OR, 0.26; 95% CI, 0.13-0.53; P < .001) and airway anomaly (OR, 0.35; 95% CI, 0.15-0.79; P = .01) were significantly associated with decreased likelihood to progress in feeding based on FOIS scores
Of the 125 patients who were tube fed at initial presentation, 20% (n = 25) were able to achieve full oral feeding after intervention
My take: While the complexity score did correlate with likelihood of progressing with oral feedings, it appears that this score is unnecessary as likelihood of progressing is mainly related to two factors: neurological comorbidities and airway anomalies.
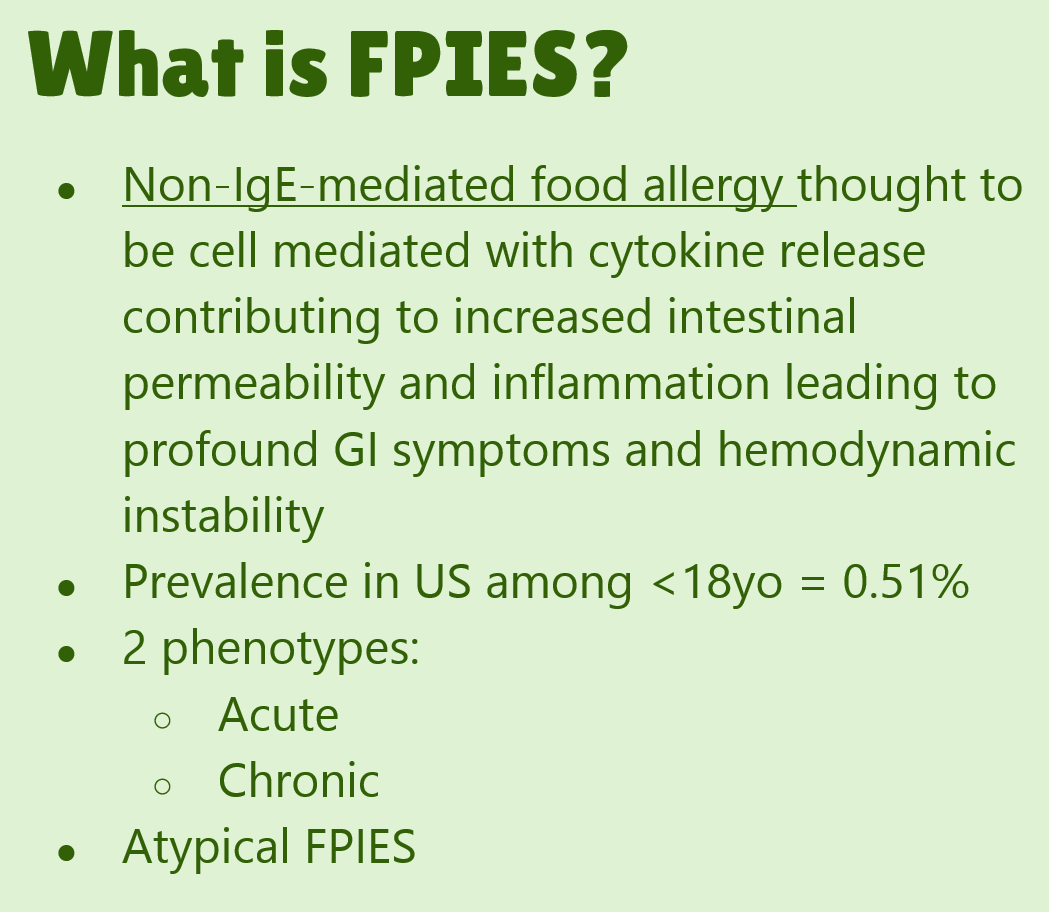
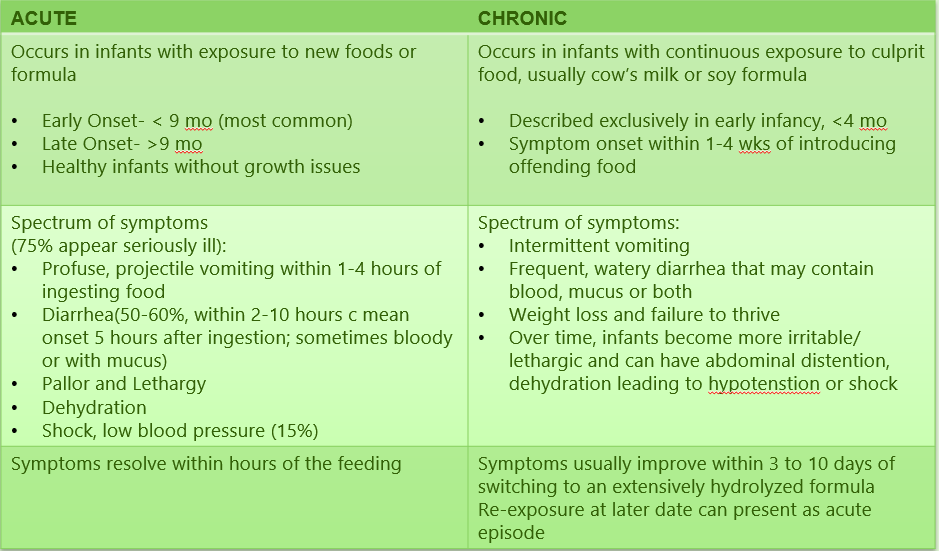
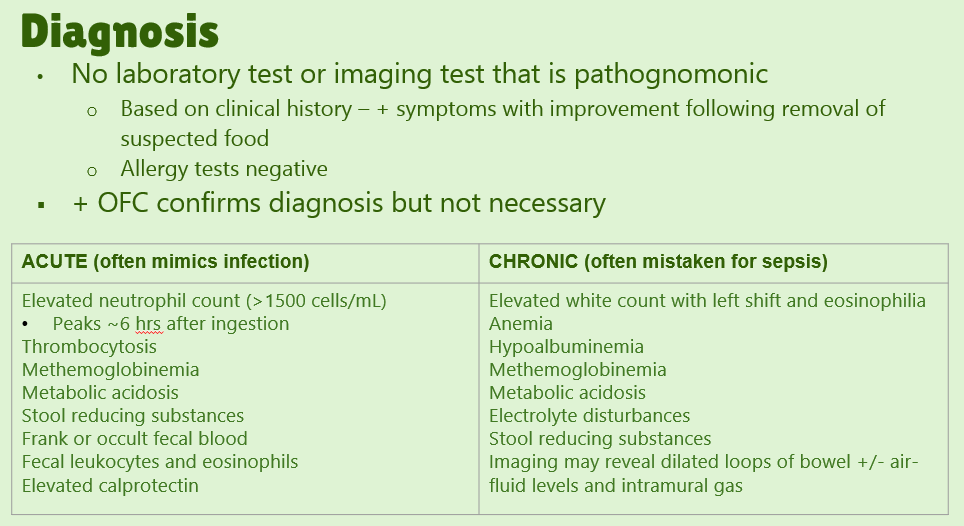
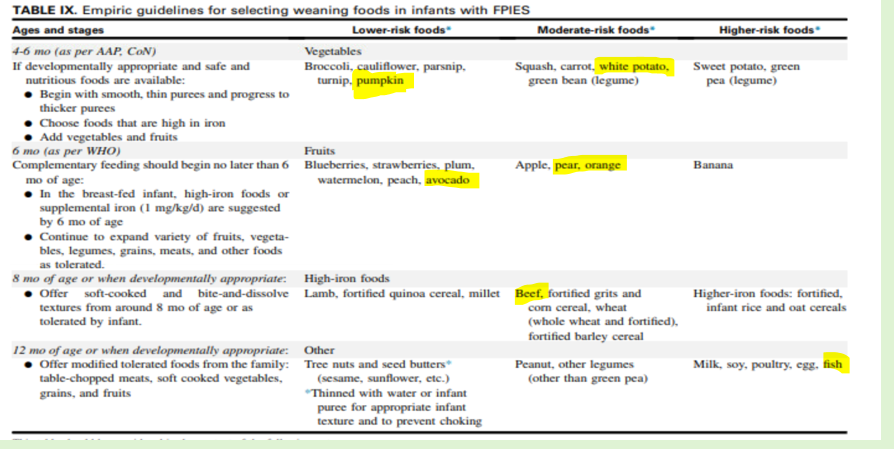
Our excellent nutritionist, Bailey Koch, recently gave our group a terrific update on FPIES. Bailey is part of the medical advisory board for THE FPIES Foundation, as is Dr. Benjamin Gold from our group. Here are many of the slides from her lecture.
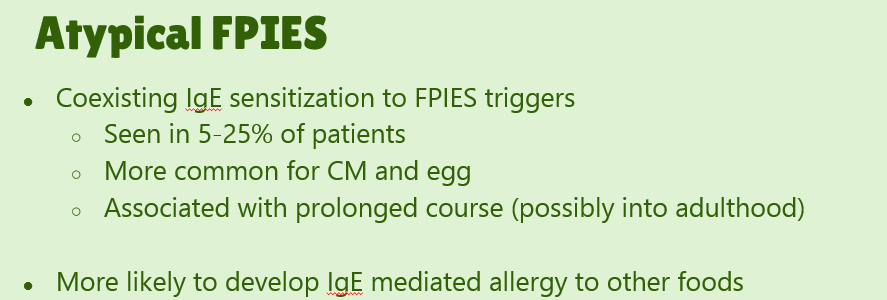
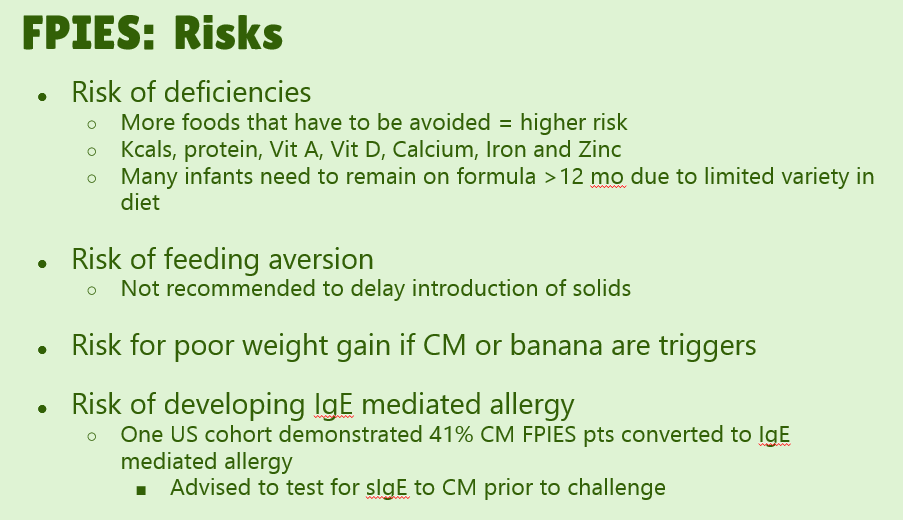
#4. “Consider specific IgE testing of children with FPIES to their trigger food because comorbid IgE-mediated sensitization to triggers, such as CM [cow’s milk], can infer a greater chance of persistent disease.
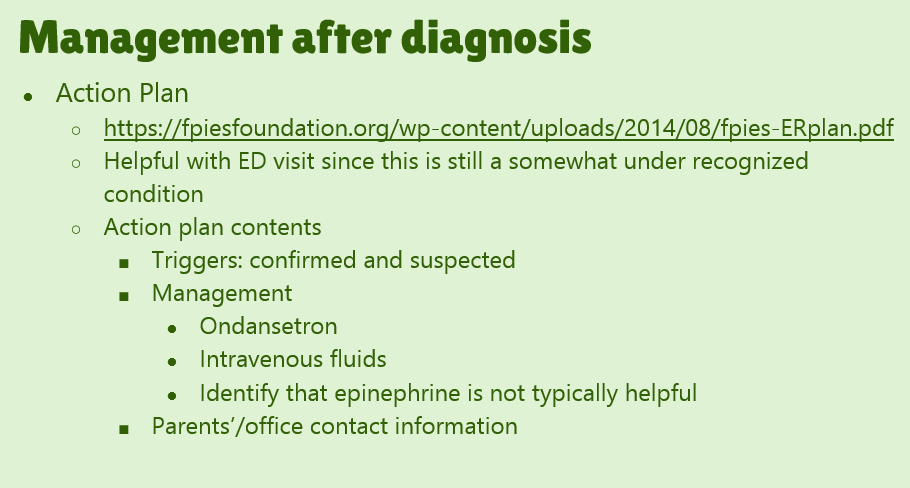
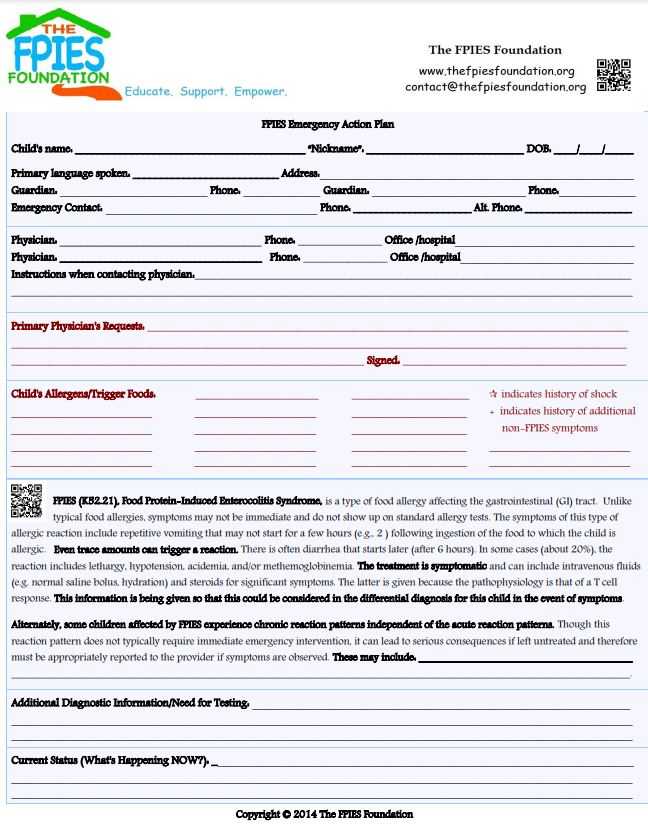
”#8. Conduct food challenges “in patients with suspected FPIES in medically supervised settings in which access to rapid fluid resuscitation is available and prolonged observation can be provided, if necessary.”
#14. Do not routinely obtain endoscopic evaluation as part of the evaluation of FPIES.
#17. Acute FPIES should be considered a medical emergency. “Approximately 15% of patients can have hypovolemic shock.”
#19. Consider ondansetron treatment as an adjunct (if >6 months of age)
#21. Do not recommend routine maternal dietary elimination of offending triggers while breast-feeding if the infant is asymptomatic.
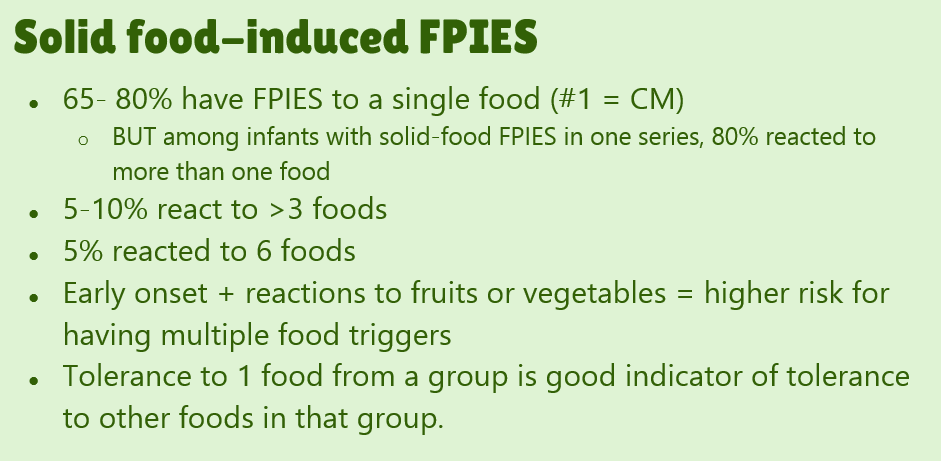
#23. FPIES can occur to multiple foods. “The majority of children (65% to 80%) have FPIES to a single food, most commonly CM.” In one study, 5% to 10% of children reacted to more than 3 foods.
#26. Use hypoallergenic formula in infants who can no longer breast-feed and are given a diagnosis of FPIES caused by CM. Most will tolerate extensively hydrolyzed formulas; some may require an amino acid based formula
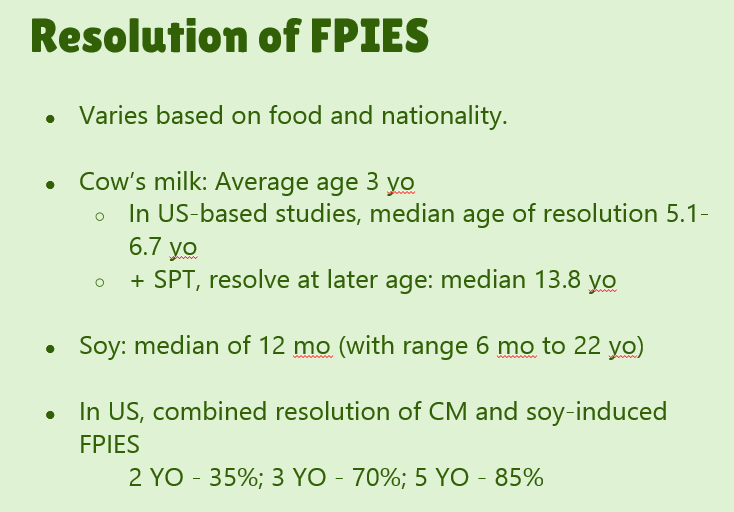
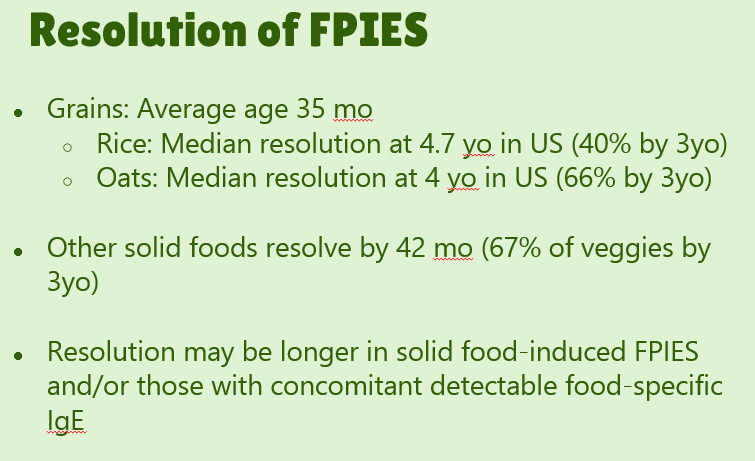
#29. Reviews natural history. “The age of CM tolerance appears to be around 3 years” but there has been variability in reports. For FPIES due to grains, average age of tolerance is 35 months and other solid foods is 42 months. The average age for soy is 12 months (later in some studies), for rice 4.7 years and 4.0 years for oats. For CM-FPIES with positive SPT response, a much protracted course has been reported, with older age of tolerance (~13.8 years)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Patients (<11 yrs old) with acute gastroenteritis (AGE, n=2503) and healthy controls (HC, n=537) old enrolled in the New Vaccine Surveillance Network study between December 2011 to June 2016. Key findings:
One or more organisms was detected in 1159 of 2503 children (46.3%) with AGE compared with 99 of 537 HC (17.3%).
Norovirus was detected most frequently among AGE (n = 568 [22.7%]). The other frequent pathogens detected were rotavirus 7.8% (despite ~75% vaccinated population), adenovirus 4.8%, C difficile 5.3%, Salmonella 6.4%, and Shigella 4.5%. 63.5% of all pathogens detected were viruses.
C difficile was detected more frequently in the HC population (7% vs 5.3%). E coli infections, likewise, were very commonly observed in the HC population (2.1% vs 1.1%). The false positive rates for C difficile pathogenicity would have been higher if the authors had not restricted their analysis to >12 months for C diff. The rates of Norovirus and Rotavirus in the HC group was 6.8% and 2.6% respectively.
Codetection of multiple pathogens was common. For example, with norovirus, 20.8% had a copathogen detected. Salmonella and C difficile had the highest codection rates of 53.5% and 54.5% respectively.
This study shows substantial improvement in rotavirus infections with a drop from 26% in detection prior to vaccine era to 6% afterwards.
My take: These muliplex molecular assays are quite useful and have improved our ability to determine underlying infections. This is particularly useful in children with underlying diseases (eg. IBD, malignancy). However, this report serves as a cautionary note that many pathogens, including C diff and E coli, are frequently identified with PCR assays in healthy children
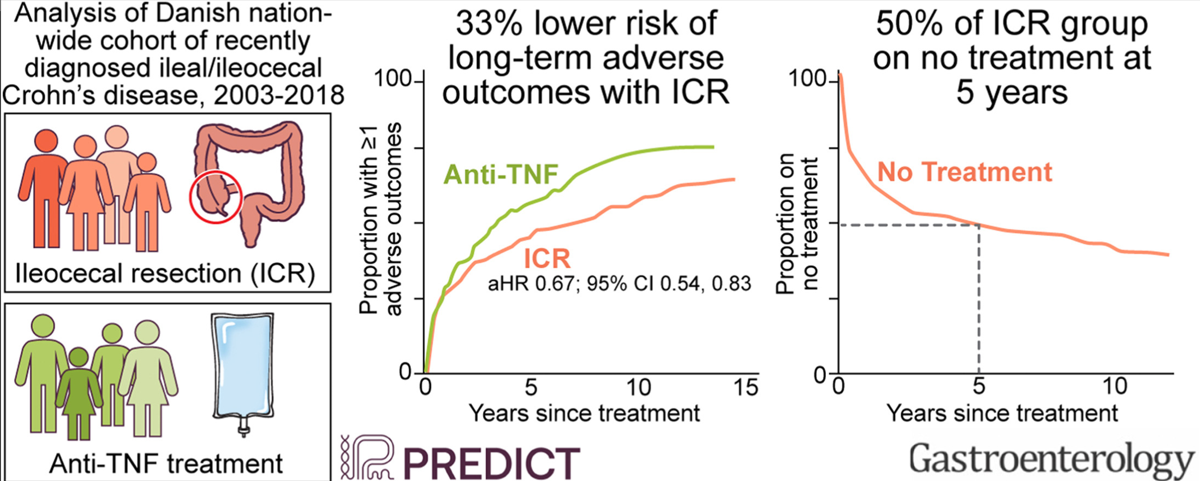
In this study from Denmark (2003-2018) using the Danish National Patient and Prescription Registries, the role of early ileocecal resection (CR), n=581, was compared with anti-TNF treatment, n=698. The primary outcome was a composite of ≥1 of the following: CD-related hospitalization, systemic corticosteroid exposure, CD-related surgery, and perianal CD. Only 178 patients (13.9%) were less than 17 years old. ICR cohort had surgery within 5 months of diagnosis in 85%, and in all within 1 yr of diagnosis. Key findings:
The risk of the composite outcome was 33% lower with ICR compared with anti-TNF (adjusted hazard ratio, 0.67; 95% confidence interval, 0.54–0.83). ICR was associated with reduced risk of systemic corticosteroid exposure and CD-related surgery, but not other secondary outcomes
Of individuals who underwent ICR, the Kaplan-Meier estimate of the proportion who postoperatively initiated IMM, initiated anti-TNF treatment, underwent another intestinal resection, or were on no treatment at 5 years of postoperative follow-up was 46.3%, 16.8%, 1.8% and 49.7%,
Of those who were initiated on infliximab as primary therapy, the Kaplan-Meier estimate of the proportion who underwent ICR, switched to a different biologic agent, or continued infliximab at 5 years of follow-up was 17.7%, 40.8%, and 47.3%
The authors note that their cohort had infrequent complicated disease: “Before ICR, 21% were diagnosed with a stricture, ileus, internal fistula, or abscess, indicative of complicated CD and representative of the real world. In contrast, only 1.7% in the anti-TNF group had complicated CD.”
My take: This study suggests that ICR may be a reasonable option in many cases of Crohn’s disease at an earlier stage rather than reserved for only those with refractory disease and complications. However, in pediatric patients, I would be more reluctant to start with a surgical approach given even longer time frame in which further surgery could be needed.
Yesterday’s post was meant to be published on Halloween –will need to fire my editor.
———-
One of the highlights of NASPGHAN’s annual meeting is the Year in Review lecture. Sandeep Gupta, the editor of JPGN, provided a fantastic review. Here are some of the slides:
In this retrospective study with 133 children (2008-2019), typical dosing of thiopurines: azathioprine 2-2.5 mg/kg/day and 6-mercaptopurine 1.5 mg/kg/day. Patients with previous or concomitant treatment with 5-ASA were allowed in the study. 62% (n=83) of the cohort had pancolitis. Key Findings:
Seventy-four patients (56%) had CS-free clinical remission at week 52 without rescue therapy
In the cohort in clinical remission, 67 and 51 patients had both CRP and calprotectin measurements at 1 year and end of follow-up. Sufficient biomarker response (CRP <1 mg/dL, calprotectin <250 mcg/g) was achieved by 44 (66%) and 44 (86%) at those two time points.
The likelihood of remaining free of rescue therapy among thiopurines-treated patients was 83%, 62%, 45%, and 37% at 1, 2, 3, and 4 years, respectively
8 of 133 (6%) stopped thiopurine therapy due to adverse effects
In their discussion, the authors make several points regarding efficacy and safety of thiopurines.
Many experts have advocated use of anti-TNF therapy agents for ulcerative colitis especially when 5-ASA medications are not effective.. This is based on higher efficacy and safety. With regard to safety, the authors note an “extremely low risk of lymphoma” citing a study from Israel in which children were followed until age of 30 years. No cases of hepatosplenic T-cell lymphoma were identified and the lymphoma rate was not statistically significant (O Atia et al. J Crohns Coliitis 2022; 16: 786-795 Open Access! Risk of Cancer in Paediatric onset Inflammatory Bowel Diseases: A Nation-wide Study From the epi-IIRN).
The authors note a recent review “rejected the hypothesis that initiation of biologic treatment later in the disease course correlates with lower response and remission rates in UC patients.”
Based on the efficacy and safety, the authors advocate for use of thiopurines “either early in the treatment course or as part of a de-escalation therapy…Thiopurines should be considered in the treatment of UC patients before the initiation of biologic drugs in most children.”
My take: In the U.S., it appears that thiopurine monotherapy, and even combination therapy, in pediatrics with IBD is used infrequently. Anti-TNF therapy with therapeutic drug monitoring is used routinely in patients if a 5-ASA is ineffective or not a good option. This article is a reminder that thiopurines are still a reasonable option. This would have been a good opportunity for a commentary in JPGN to add some context to this article regarding the role of these agents.
AGA guidelines for moderate-to-severe ulcerative colitis: “In adult outpatients with moderate to severe UC in remission, AGA makes no recommendation in favor of or against using biologic monotherapy or tofacitinib rather than thiopurine monotherapy for maintenance of remission.”
Most fundic gland polyps (FGPs) are small (0.1 to 1 cm) sessile polyps characterized histologically by cystic oxyntic glands with a mixture of parietal cells and chief cells.
Most FGPs are “sporadic” and associated with chronic PPI use. These are benign.
Syndromic FGPs are associated with familial adenomatous polyposis (FAP) and have a “0.6% lifetime risk of progressing to gastric carcinoma.” 73% of syndromic FGPs had low-grade dysplasia in one study.
Routine excision of FGPs is not recommended in the absence of high-risk features (see below)
In Figure 1, the authors outline an algorithm for surveillance:
Sporadic: If FGPs are thought to be sporadic and have no dysplasia, no follow-up is needed. If FGPs are thought to be sporadic, but have dysplasia, “consider diagnostic workup for syndromic FGP.” “Surveillance by EGD of sporadic FGPs with our without low-grade dysplasia is not routinely recommended, as progression to gastric cancer is rare… In patients with multiple FGPs (eg. carpeted polyposis), large (>1 cm) polyps, or the presence of high-grade dysplasia, FAP needs to be ruled via genetic testing and colonoscopy.”
Syndromic: If low risk FGP, then surveillance recommended beginning at 25 years of age. If high risk FGP, surveillance is recommended every 1-2 years. High-risk features include multiple FGPs (eg. carpeted polyposis), large (>1 cm) polyps, or the presence of high-grade dysplasia
In this review, the authors recommend VCE for Peutz-Jeghers syndrome no later than 8 years of age; for constitutional mismatch repair deficiency, the authors recommend “consider VCE surveillance before age 10.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
#2: Treatment options for supragastric belching may include brain–gut behavioral therapies, either separately or in combination, such as cognitive behavioral therapy, diaphragmatic breathing, speech therapy, and central neuromodulators.
#6: Abdominal imaging and upper endoscopy should be ordered in patients with alarm features, recent worsening symptoms, or an abnormal physical examination only.
#7: Gastric emptying studies should not be ordered routinely for bloating and distention, but may be considered if nausea and vomiting are present. Whole gut motility and radiopaque transit studies should not be ordered unless other additional and treatment-refractory lower gastrointestinal symptoms exist to warrant testing for neuromyopathic disorders.
#10: Probiotics should not be used to treat abdominal bloating and distention.
#11: Central neuromodulators (eg, antidepressants) are used to treat bloating and abdominal distention by reducing visceral hypersensitivity, raising sensation threshold, and improving psychological comorbidities.
Gastric belching: tracing showing instead a distal to proximal increase in impedance with air clearing from the esophagus. Arrows indicate direction of air flow and high-resolution manometric view of gastric belching is shown with direction of air flow from stomach to upper esophagus seen (orange arrow)
Several points from review:
Belching can be from the esophagus or from the stomach.
Supragastric belching involves air clearing from the esophagus not from stomach and is frequently associated with anxiety.
Gastric belching is frequently associated with reflux and occurs after spontaneous transient relaxation of the lower esophageal sphincter.
Bloating is a subjective sensation of fullness, tightness or trapped gas. Food intolerances, bacterial overgrowth, and celiac disease need to be considered. If constipation is present, this should be treated.
My take: This is a good review with plenty of practical suggestions for management.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Lately, I have been struck by the increasing volumes of research on disparities in medicine. A recent issue from the Journal of Pediatrics had at least 4 articles touching on this subject. Most of these articles view these disparities as being due to structural racism.
In this article, the authors show that among 519 children with newly diagnosed IBD, black patients were less likely to achieve CSFR (corticosteroid-free remission) 1-year post diagnosis (OR: 0.52, 95% CI:0.3-0.9) and less likely to achieve sustained CSFR (OR: 0.48, 95% CI: 0.25-0.92). This was despite a similar phenotype. Black patients had much higher rate of public insurance (58% vs 30%) and were less likely to be seen for routine follow-up visits.
While the authors attribute the response to therapy as likely to be related mainly to social determinants of health, there may be biologic factors at work as well. In a recent study (R Greywoode et al. Inflamm Bowel Dis 2023; 29: 843-849. Open Access! Racial Difference in Efficacy of Golimumab in Ulcerative Colitis), there were disparate racial response rate differences among patients receiving the same therapy.
In this retrospective review of 38,334 specialty referrals (2019-2021), of all referrals, 62% were scheduled and 54% were completed. Referral completion rates were lower for patients with Black race (45%), Native Hawaiian/Pacific Islander race (48%), Spanish language (49%), and public insurance (47%). Since the report focused on primary clinics within 5 miles of the hospital, the authors indicate that the lower referral completion is due to nongeographic structural barriers, including problems with arranging visits as some families have less flexible jobs. The authors conclude that the fact that specialty care is inaccessible is due to ” the effects of racism and discrimination on the scheduling process.” The authors recommend that the referral workflows should not “place the administrative onus of scheduling exclusively on families.”
This was a retrospective cohort analysis of linked birth and death certificates from 50 states from 2005 to 2014 to investigate among US infants born at <37 weeks gestation (a) racial and ethnic disparities in sudden unexpected infant death (SUID). Key findings:
Among 4,086,504 preterm infants born during the study period, 8096 infants (0.2% or 2.0 per 1000 live births) experienced SUID. State variation in SUID ranged from the lowest rate of 0.82 per 1000 live births in Vermont to the highest rate of 3.87 per 1000 live births in Mississippi
In the adjusted analysis (for sociodemographic and clinical factors), compared with Non-Hispanic white infants, Non-Hispanic black infants and Alaska Native/American Indian preterm infants had greater odds of SUID (aOR, 1.5)and aOR, 1.44)
The authors attribute the adjusted differences to “structural racism [that] creates and perpetuates health inequities.”
This was a retrospective cohort study of 3290 infants hospitalized in a single center NICU between 2017 and 2019 in the Racial and Ethnic Justice in Outcomes in Neonatal Intensive Care (REJOICE) study. Key findings:
205 families (6.2%) that experienced an adverse social event. Black families were more likely to have experienced a CPS referral and a urine toxicology screen (OR, 3.6). American Indian and Alaskan Native families were also more likely to experience CPS referrals and urine toxicology screens (OR, 15.8 and OR, 7.6)
Black families were more likely to experience behavioral contracts and security emergency response calls
My take: These articles offer more proof that racial disparities are highly prevalent in healthcare. While we should strive to help improve access/equitable care in medicine, the approach needs to start well before the clinic/hospital. To make the greatest impact, policies are needed to address education outcomes and poverty (eg. expanded child income tax credit) which overall impact health more than anything that happens in our clinics.
Safe Sleep A terrific website that focuses on this crucial issue: Charlieskids.org; it has videos, do’s and don’ts as well as a link to Cribs for Kids (discounted safe crib website). In addition, this website has a book called “Sleep Baby Safe and Snug” which incorporates updated recommendations on safe sleep practices.
The High Toll of Sudden Infant Death From 2013-2015, there was an average of 3523 US infants each year who died from SUID (sudden unexpected infant death), peaking at 1-2 months of life. More black infants died of SUID in the first year than black children who died from firearm homicides in all of childhood through age 19 years. SUID deaths from 2013-2015 (10,568) was similar to the total number of motor vehicle-traffic deaths in all of childhood (10,714) and greater than the total number of any of the other causes.