Thanks to all of you who provided articles, suggestions and encouragement to make this blog better this past year. This has been the 12th year for this blog and it has continued to gain more views each year. Here are links to many of my favorite posts from 2023 along with a few pictures:
In pediatrics, there is often a prevailing view that kids can overcome a lot due to their resiliency. However, just like a a track event, if you trip or fall back in a race, you may never catch up. With many medical conditions, it is unclear whether a delay in diagnosis results in long-term deficits. Recent data have found that a ~1 month delay in the treatment of cystic fibrosis is associated with poorer nutritional/growth outcomes, even 5 years later.
Using the U.S. Cystic Fibrosis Foundation patient registry (CFFPR), the authors examined children born between 2010-2018 who were diagnosed based on newborn screening (NBS). Age at first event (AFE) serves as a proxy for when CF care was likely initiated. Patients were divided into 3 cohorts based on AFE: <14 days (early cohort), 14 days to <33 days, and 33 days or more (late cohort).
Key findings:
Infants in the late cohort were more likely to have a sweat test as their first CF event.
Pulmonary exacerbations were reported as the reason for hospitalization in in 59.1% of late cohort compared with 4.8% of early cohort with hospitalization as their first CF event.
Height-for-age z-scores were consistently lower in the late cohort. At 1 yr and 5 yrs, median z-scores were -0.6 (vs. -0.42) and -0.26 (vs. -0.12 in early group) respectively
The authors note that the early and late groups had differences in parental education attainment which “may be evidence that the late cohort had lower socioeconomic status that could have resulted in barriers to timely evaluation.”
The discussion notes that the introduction of highly effective modulator therapy does not overcome early stunting; which indicates that even with newer therapy, institution of nutritional treatments remains critical.
The study confirms that
NBS/early identification has clear benefits.
There is a need to quickly get suspected patients seen by CF centers.
My take: There was persistently (through at least 5 yrs) reduced height-for-age z-scores in patients with CF who presented just 27 days later.
Dr. Burrell noted that concerns for EoE are increased in those who have more uniform problems with increased textures (rather than selectivity) and in those with more severe feeding disordersSometimes Caregivers will contribute to nutritional disorders by placing on diets like a gluten-free, casein-free diet
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Before reviewing today’s article, I wanted to make a comment about the blog post on 12/17/23 (Endoscopy of the Ileal Pouch Anal Anastomosis) which was a JPGN topic of the month. The editorial staff encourages author-driven communication and author-driven initiatives for these types of articles. If you have a topic for JPGN, please send an email to the Section Editor Darla Shores (dshores1@jhmi.edu) or to the editor Sandeep Gupta. (skgupta@uabmc.edu). This includes articles that you would like to write (fellow/interested faculty with senior faculty, up to 5 authors, 1500 words, 12 references), or if you have a topic that you would like to see in JPGN but do not wish to write yourself, please inform the editorial team as well.
In this retrospective review, pediatric patients (n=25) received intrapyloric botox injections: (80-100 IU divided into 4 doses administered via sclerotherapy needle.
Key findings with botox injections:
Of 22 patients completing a GE study, 14 had delayed GE with no significant difference between IPBI responders and nonresponders
Improvement in vomiting in 80% (16/20), nausea 75% (15/20), abdominal pain 79% (15/19).
In those with psychiatric diagnosis, improvement was seen 71%. In those with orthostatic intolerance, improvement was noted in 67%.
In those with delayed GE, improvement was noted in 79% compared with 63% (5/8) with normal GE
My take: Botox was associated with improvement in this refractory pediatric group regardless of gastric emptying/manometry. This suggests that relaxation of pylorus is a useful therapeutic modality in a subset of patients.
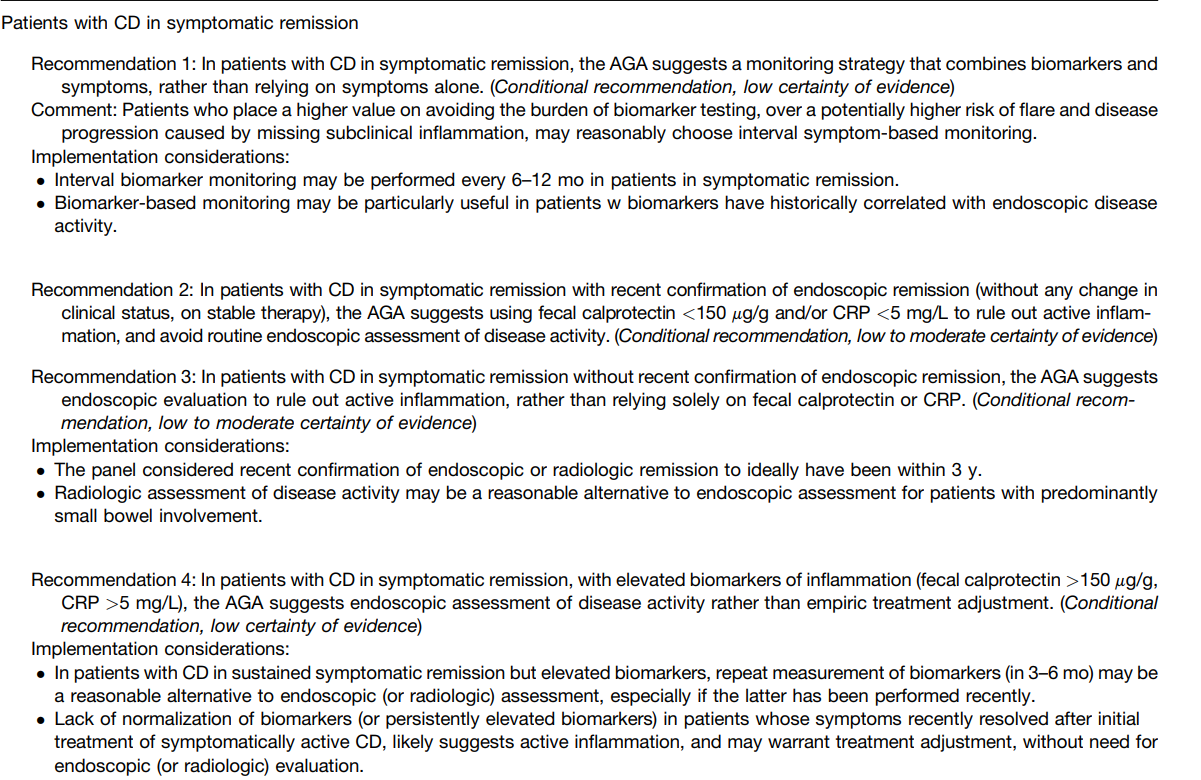
Recommendation #2: In patients in symptomatic remission with recent endoscopic evaluation (w/in 3 yrs), a fecal calprotectin <150 μg/g and normal CRP rules out active inflammation, avoiding endoscopic evaluation for assessment of disease activity. However, elevated biomarkers in this setting merit confirmation with endoscopy before treatment adjustment.
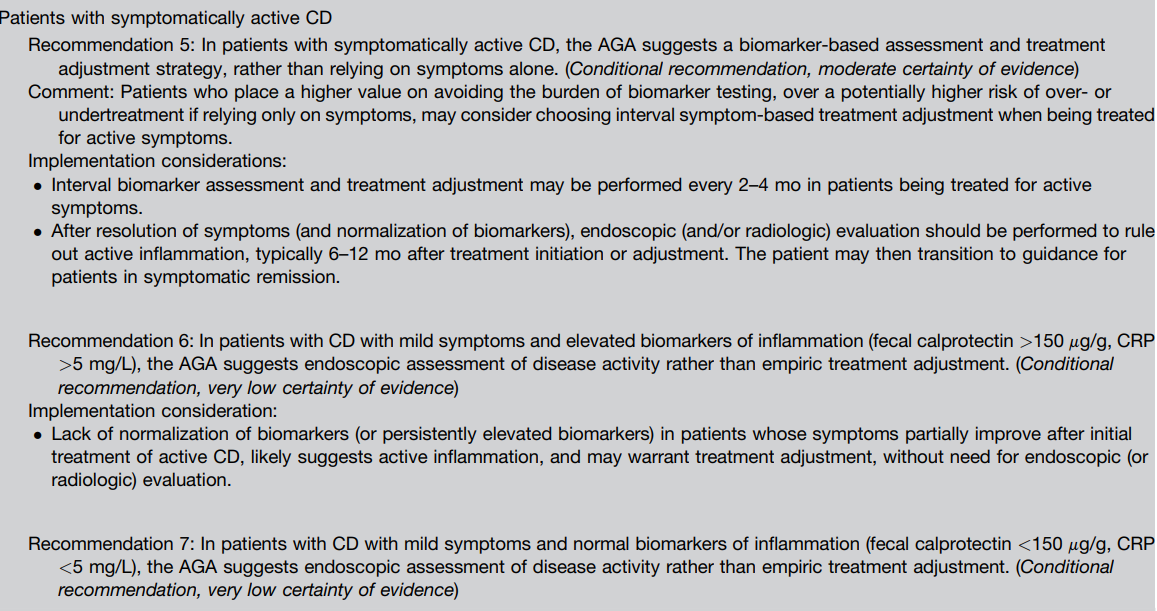
Recommendations #6, #7: In patients with CD with mild symptoms, neither normal nor elevated biomarkers alone are sufficiently accurate to determine endoscopic activity.
Recommendations #8, #9: In patients with CD with moderate to severe symptoms, elevated fecal calprotectin or serum CRP suggests endoscopic activity, precluding routine endoscopic assessment for disease activity. In those with moderate to severe symptoms but normal biomarkers, endoscopic assessment is recommended rather than empiric adjustment in treatment.
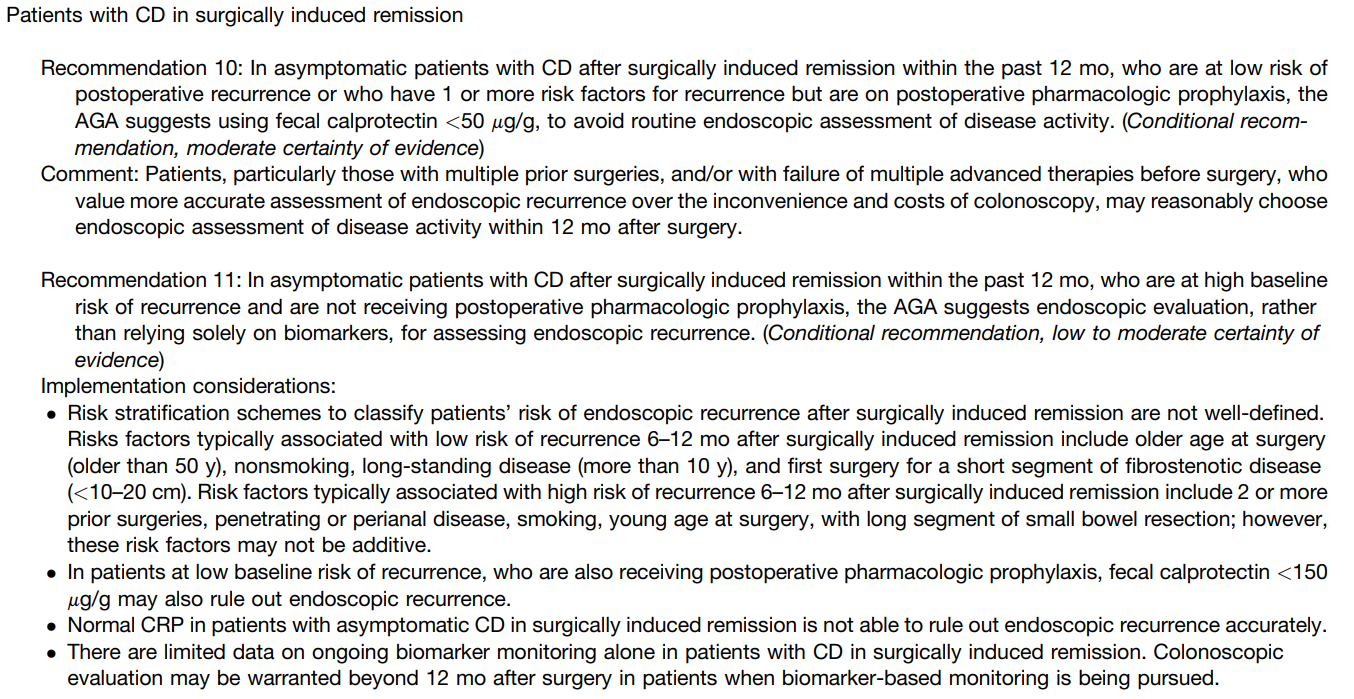
Recommendation #10: In patients with CD in surgically induced remission in low-risk patients on pharmacologic prophylaxis, a normal fecal calprotectin (<50 mcg/gm) reliably rules out endoscopic recurrence.
More Recommendations:
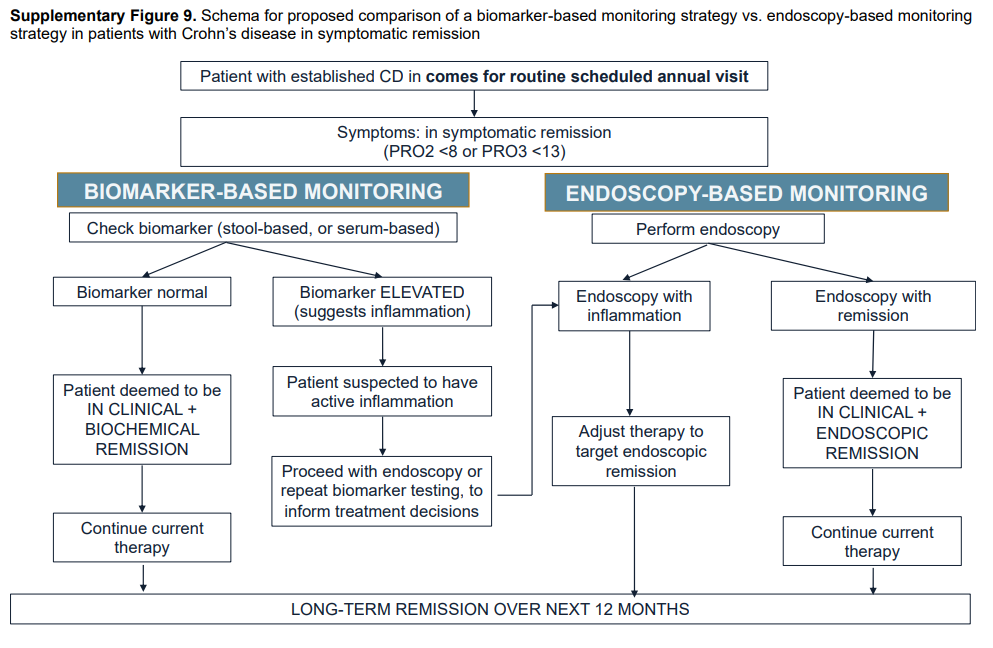
#1 In patients with CD in symptomatic remission, the AGA suggests a monitoring strategy that combines biomarkers and symptoms, rather than relying on symptoms alone.
#3 In patients with CD in symptomatic remission without recent confirmation of endoscopic remission, the AGA suggests endoscopic evaluation to rule out active inflammation, rather than relying solely on fecal calprotectin or CRP.
#5 In patients with symptomatically active CD, the AGA suggests a biomarker-based assessment and treatment adjustment strategy, rather than relying on symptoms alone.
My take: This practical guidance will help target endoscopy in patients with Crohn’s disease. In those who are feeling well with normal biomarkers, frequent endoscopic evaluation is a low-value procedure. Similarly, in those with very elevated biomarkers and who are very symptomatic (with normal infectious studies), endoscopic evaluation is often unnecessary. The AGA expert recommendations should help persuade insurance companies to include biomarkers in their coverage.
Summary of all recommendations -see below from Figure 9 and Table 3.
This is a terrific review with some good pictures.
The authors note that in their practice in their IBD center, a pouchoscopy is performed 1-2 years after ileostomy closure irrespective of symptoms; in those with symptoms, it is performed sooner.
Some complications like strictures and ulcers can occur with few symptoms
Table 1 reviews common complications like strictures, cuffitis, infectious pouchitis, Crohn’s disease like pouch inflammation, pouch ischemia, and irritable pouch syndrome. Figure 2 provides useful endosopic picture
Background: “Despite their [5-aminosalicylates (5-ASA)] lack of efficacy in Crohn disease (CD), they are still used in real-world practice.”
Methods: In this pediatric retrospective study with 61 patients with ileocolonic disease, 24 received concomitant immunomodulator therapy.
Key findings:
The majority of patients (85%) required escalation to biologics. 71% of those receiving an immunomodulator required escalation to a biologic and all but 35 of 37 on mesalamine monotherapy required escalation to a biologic
There was no difference between those who continued 5-ASA at time of biologic initiation compared to those who did not continue the medication
Patients who discontinued 5-ASA had an average annual cost savings of $6741
My take: In those with very mild Crohn’s disease, the best option may be a dietary approach. Mesalamine therapy remains a good option in patients with ulcerative colitis.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
More amazing stone work on walking areas in Lisbon
NASPGHAN has developed a useful ~6 minute video for families reviewing the treatments (diet and medications) for eosinophilic esophagitis. When I visited the site, it had not garnered much traction yet (very few views). I would recommend this video to families:
This is a terrific review of the dysphagia and the multidisciplinary approach to management. Many pearls are in this article. For example, laryngo-tracheo-esophageal cleft (LTEC), “while rare, 1 in 10,000-20,000 live births, the incidence of LTEC is higher (7.6%-22%) in children with aerodigestive issues such as a chronic cough.” [As an aside, this should be repeated given the changing population of patients being seen.]
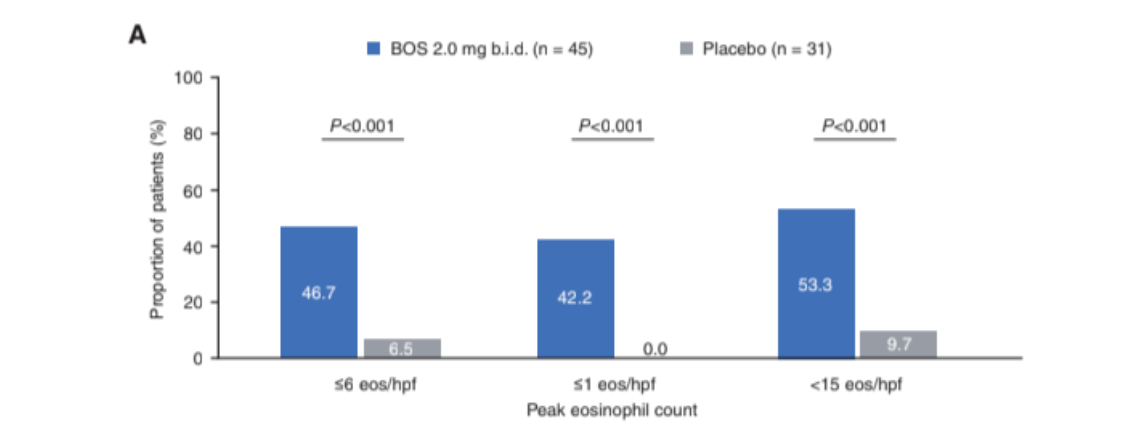
Key finding: Significantly more patients who received BOS (2mg BID) than placebo achieved histologic responses (≤6 eos/hpf: 46.7% vs 6.5%; ≤1 eos/hpf: 42.2% vs 0.0%; <15 eos/hpf: 53.3% vs 9.7%; P < 0.001)