Recently, Dr. Shruthi Arora, an Emory Pediatric Endocrinologist and part of CHOA’s Strong4Life team, provided a terrific review of pediatric obesity pharmacology for our group.
Here are a few slides from Dr. Arora’s lecture:
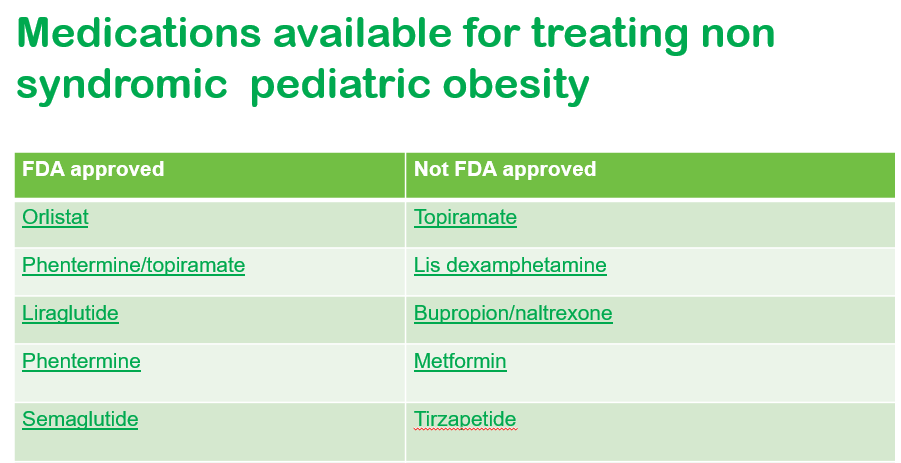


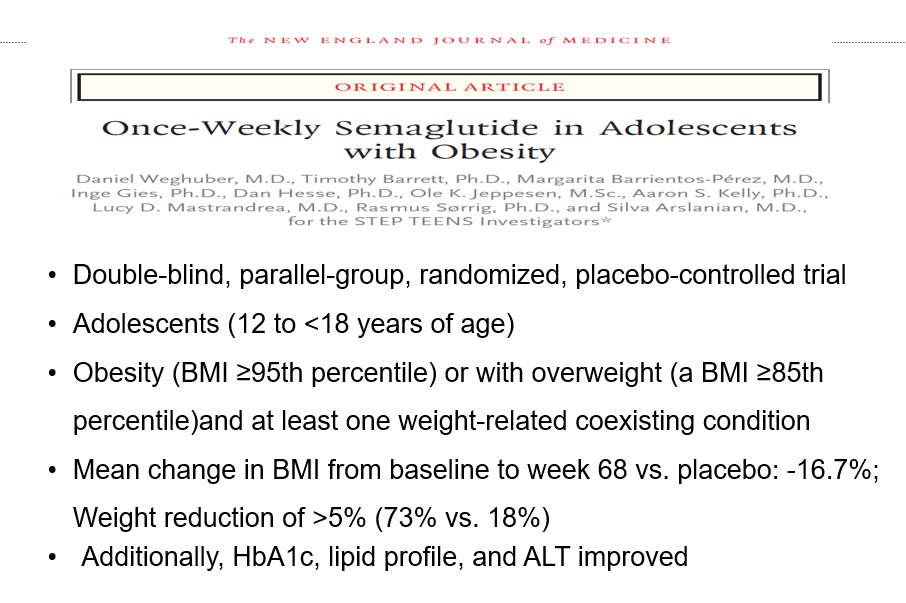
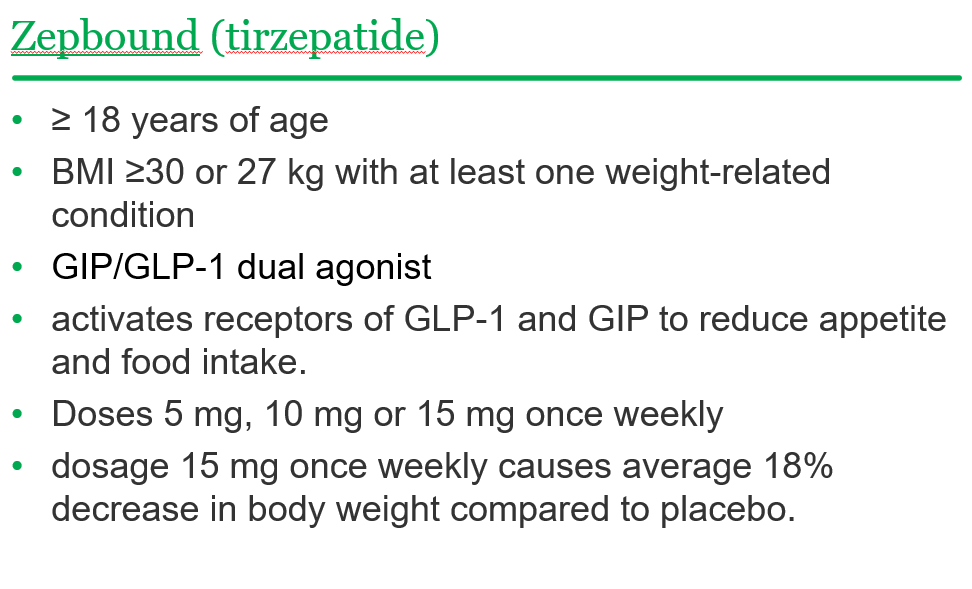


General points from this lecture:
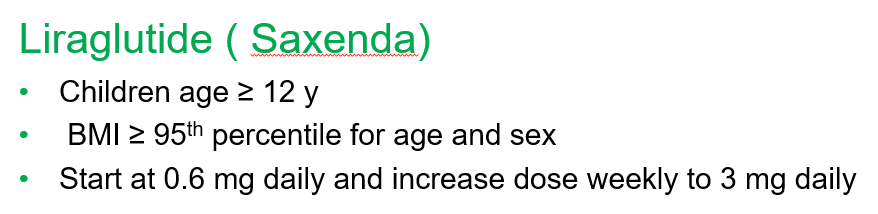
- GLP-1 agents are a huge advance but currently limited by affordability (frequently there is a lack of insurance coverage if there is not T2DM) and availability. In addition, most individuals will regain weight loss when these agents are stopped.
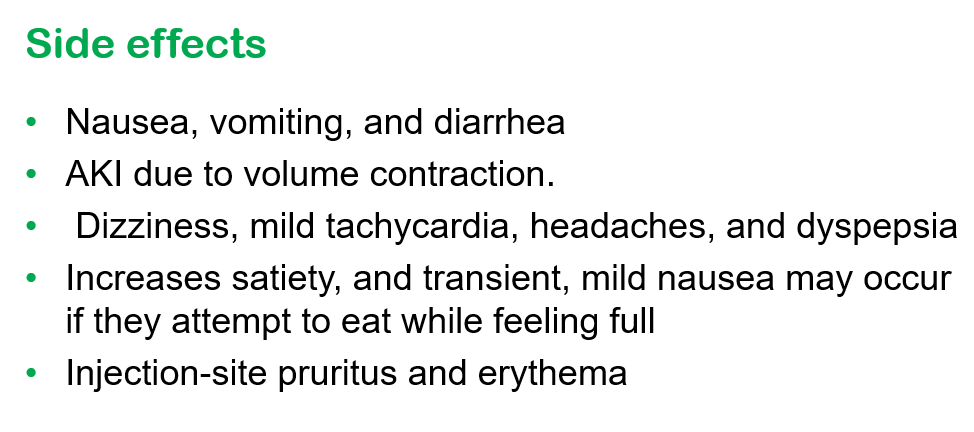
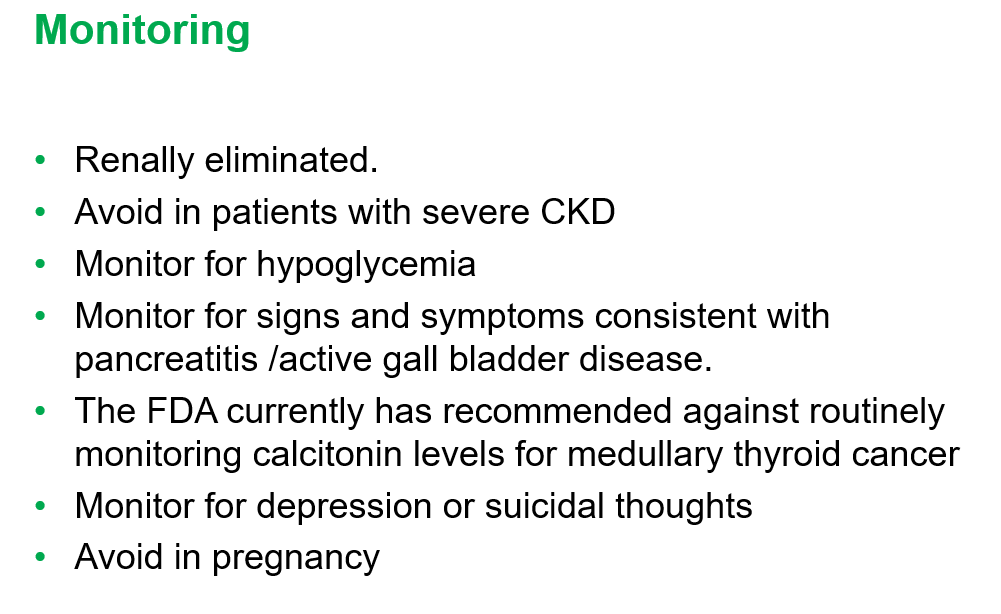
- GLP-1 agents are not recommended in the following: patients with gastroparesis, and patients with a personal or family history significant for MEN 2 A /MEN 2 B/ Medullary thyroid cancer
- Long-term data is still needed. These agents have been associated with muscle and bone loss; thus, working to assure a good diet is still very important
——————————————————————————
NASPGHAN has a good review/webinar on this topic as well: Pediatric MASLD in the Current Era of Pharmacological and Surgical Obesity Treatment Options. For members, after sign in, you can register and login to this webinar (look under clinical practice tab). This webinar made a lot of useful points (many covered by Dr. Arora too).
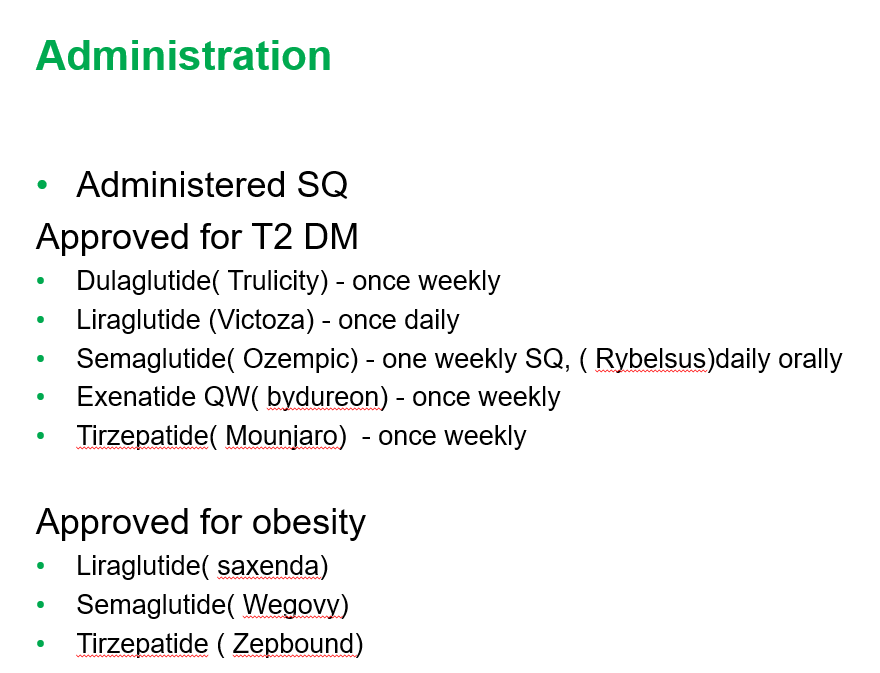
- For GLP-1 agents, due to effects on gastric emptying, they are generally held prior to anesthesia. If they are given weekly, then hold 1 week prior to anesthesia. If it is a daily medication, hold for 1 day prior to anesthesia.
- Surgery definitely helps improve MASH -though variable responses in patients. SLEEVE gastrectomy is currently the most frequent bariatric surgery
- There is trouble getting GLP-1 medications.
- Limited knowledge regarding long-term effects of cycling of GLP-1 agents.
- Obesity is a long-term disease –>anticipate long-term treatment
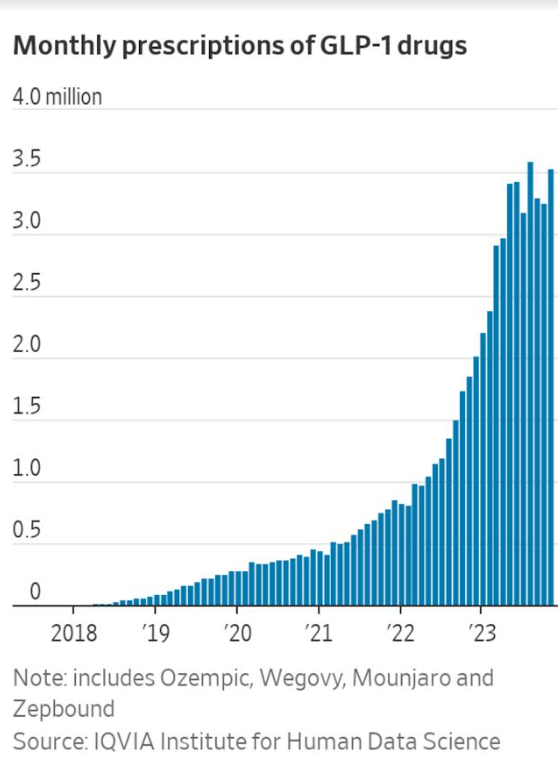
The Wall Street Journal recently published a personal account of using the newer obesity medications. Bradley Olson, 1/12/24: A Weight-Loss Drug Changed My Life. Will It Solve My Problem? (behind a paywall). This article discusses the dramatic improvement experienced by the writer along with his concerns about the cost of the medication and potential for rebound when he can no longer afford it. Two of the figures:

Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.