Vermeire S et al. Lancet 2017; 389: 266-75. The “FITZROY ” study examined clinical remission in patients with moderate-to-severe Crohn’s disease treated with filgotinib, a orally administered selective JAK inhibitor. This agent is 30 times more selective fo rJAK1 over JAK3. This study enrolled 174 patients in a phase II study. Key findings:
- Among patients naive to anti-TNF agents, clinical remission (based on CDAI <150 at week 10) noted in 47% of filgotinib-treated compared with 23% of placebo group (P=.0077)
- Among patients naive to anti-TNF agents, clinical response was noted in 67% of filgotinib-treated compared with 44% in the placebo group.
H Singh et al. Gastroenterol 2017; 153: 430-8. Using the large Manitoba Epidemiology Database with 1.3 million population (2005-2014), the authors found that individuals with IBD had a 4.8 fold increase risk of Clostridium difficile infection.
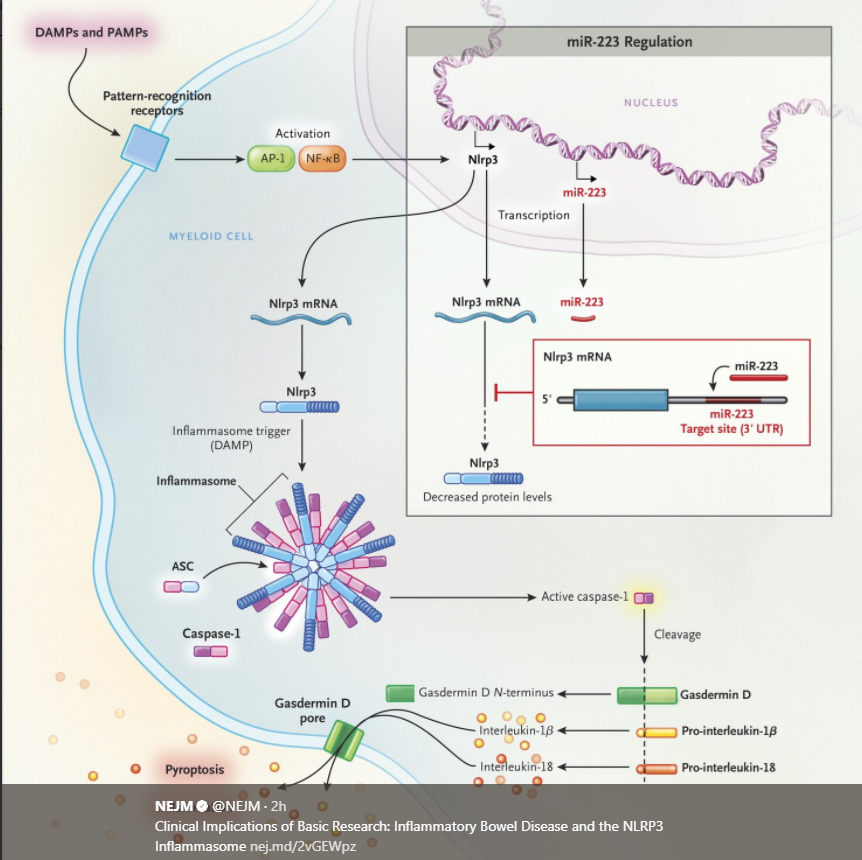
T-D Kanneganti. NEJM 2017; 377: 694-6. This review examined the NLRP3 Inflammasome. Neudecker et al (J Exp Med 2017; 214: 1737-52) identified microRNA miR-223 which functions “to suppress the Nlrp3 inflammasone during acute colitis.” Other useful points in this review of basic research:
- “The majority of the immune cells in the body are located in the intestine, where they are spatially separated from more than 10 trillion microorganisms by a layer of mucus and a layer of epithelial cells. Deterioration of this physical barrier …underlies inflammatory bowel disease.”
- miR-223 is increased in the inflamed colon. “During inflammation, the expression of miR-223 is also upregulated..and the molecule binds to its complementary sequence in a regulatory part of Nlrp3 mRNA…lead[ing] to decreased Nlrp3 expression and the consequent dampening of interleukin-1β maturation and associated inflammation.”