
Here are some selected slides and notes from this year’s NASPGHAN’s postrgraduate course. My notes from these lectures may contain errors of omission or transcription.
Link to the full NASPGHAN PG Syllabus 2019 (Borrowed with permission)
9:00 – 10:20 “Potpourri”
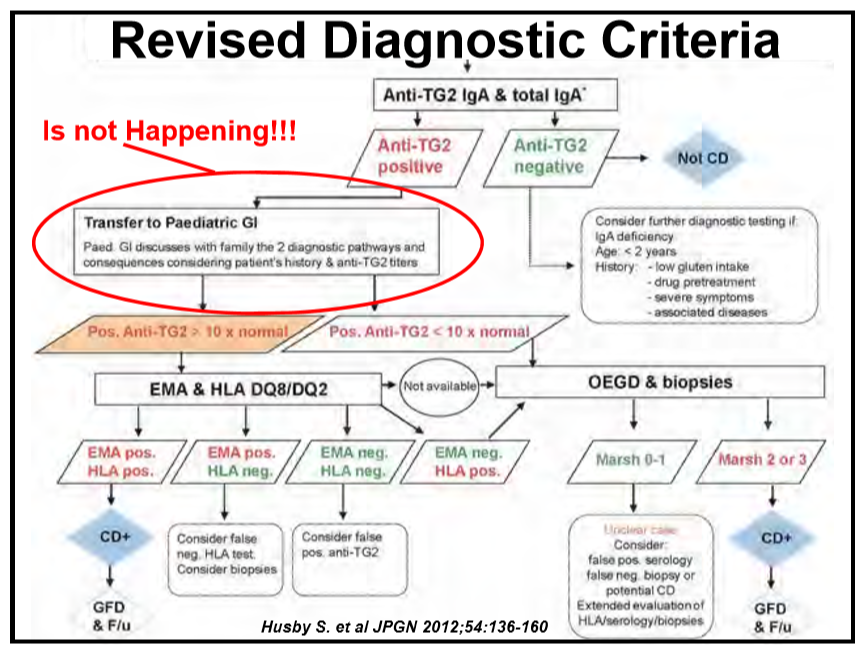
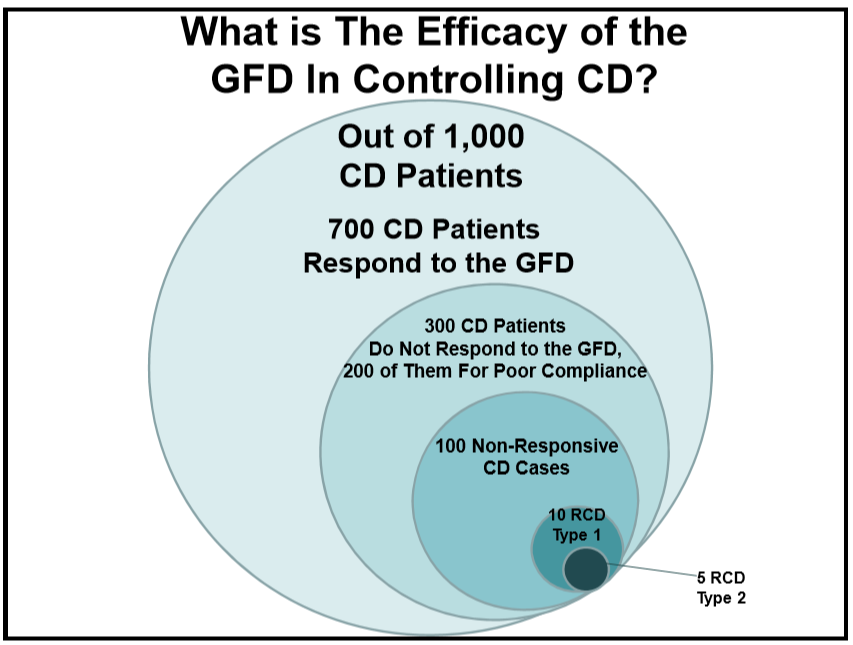
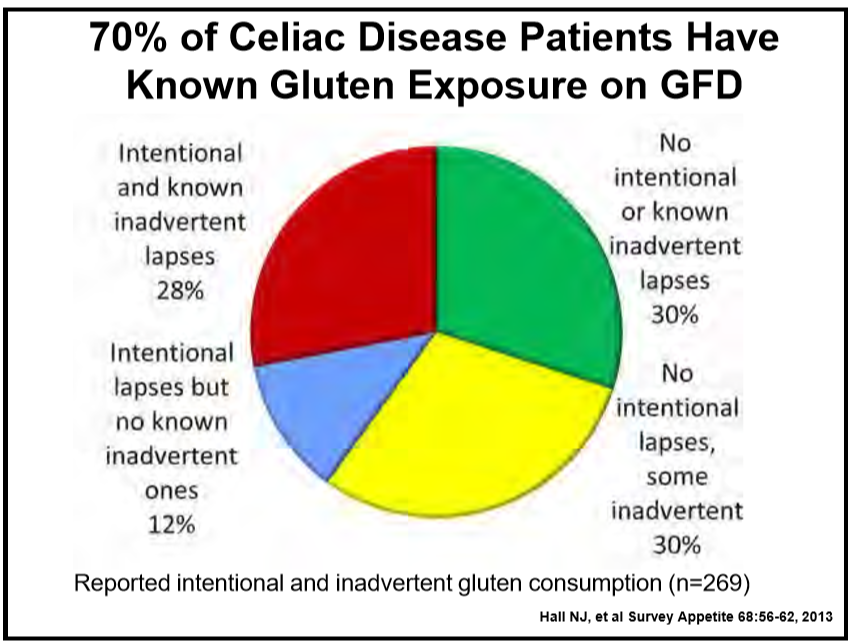
46 Alessio Fasano, MD, MassGeneral Hospital for Children Celiac disease: Beyond diagnosis
- Reviewed potential non-biopsy option for diagnosis if anti-TG2 >10 x normal. Pediatricians are not following recommendations –>many children placed on gluten-free diet at lower titer antibody-positivity.
- Recommends checking Hepatitis B antibody because many children with celiac disease do not seroconvert.
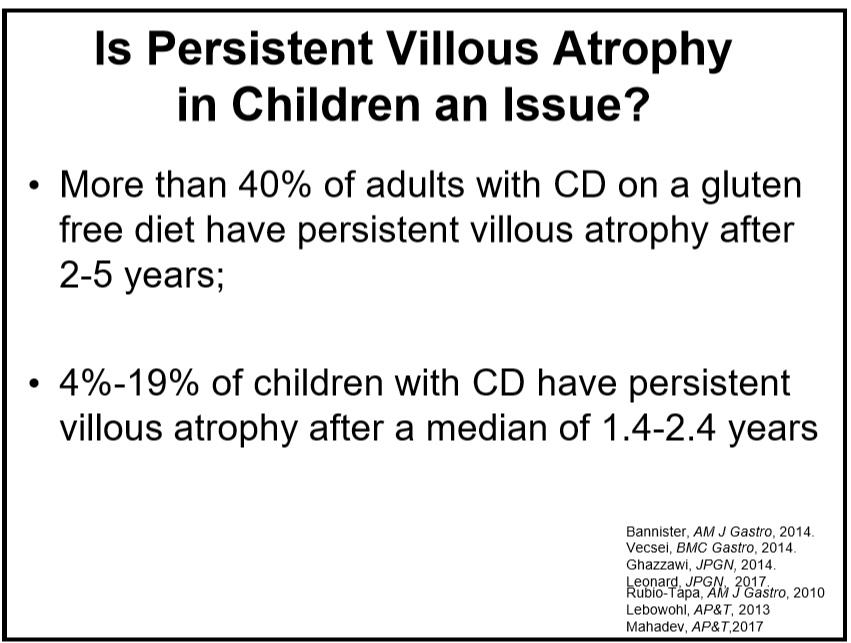
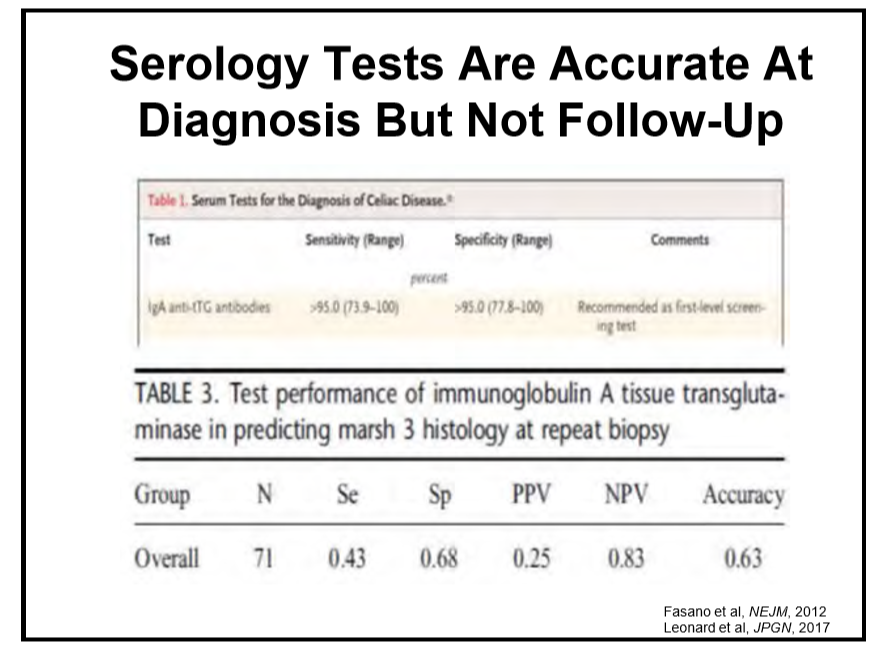
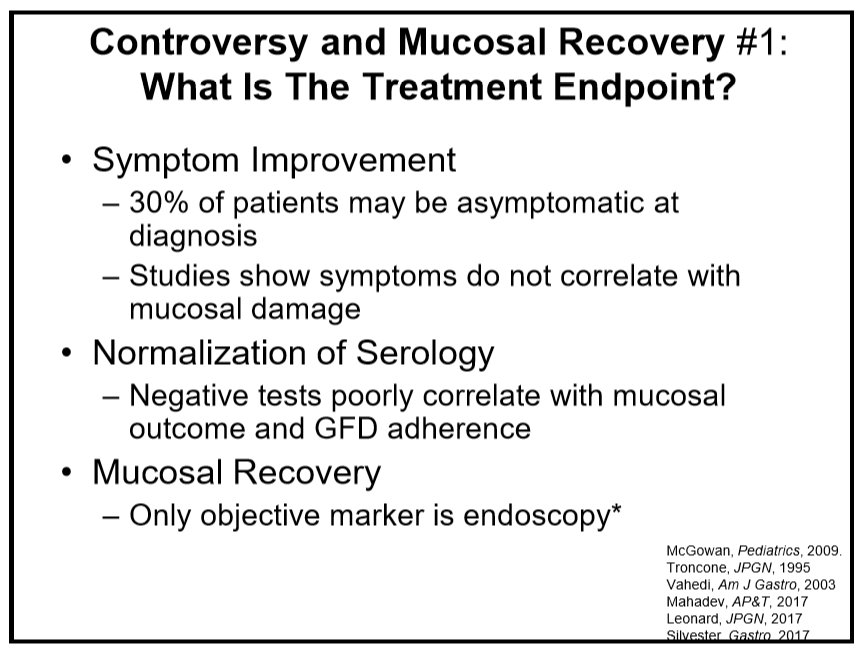
- TTG levels are good for diagnosis but not as helpful for monitoring after diagnosis.
- Only 10 out of 1000 are true refractory, about 100 out of 1000 are exquisitely sensitive to gluten

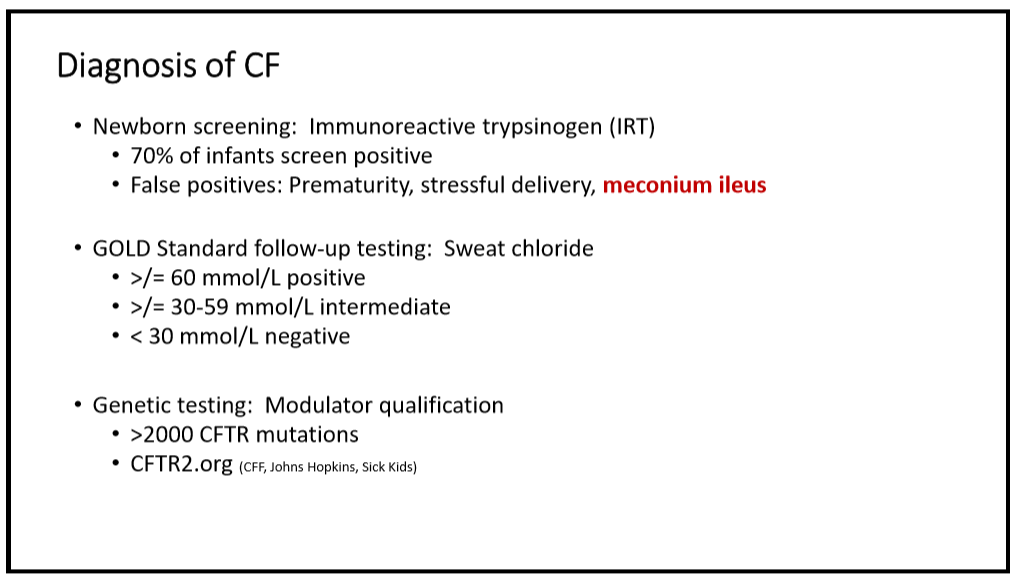
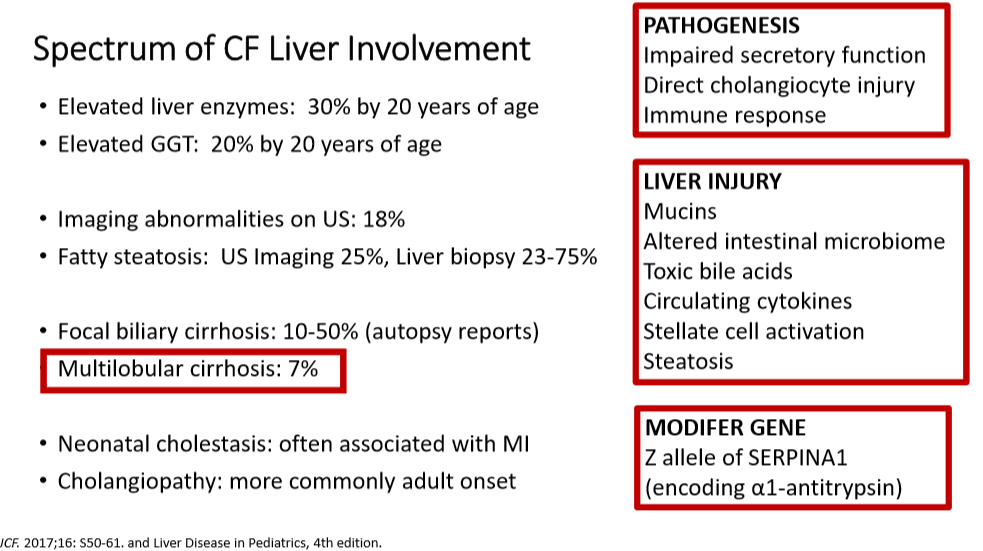
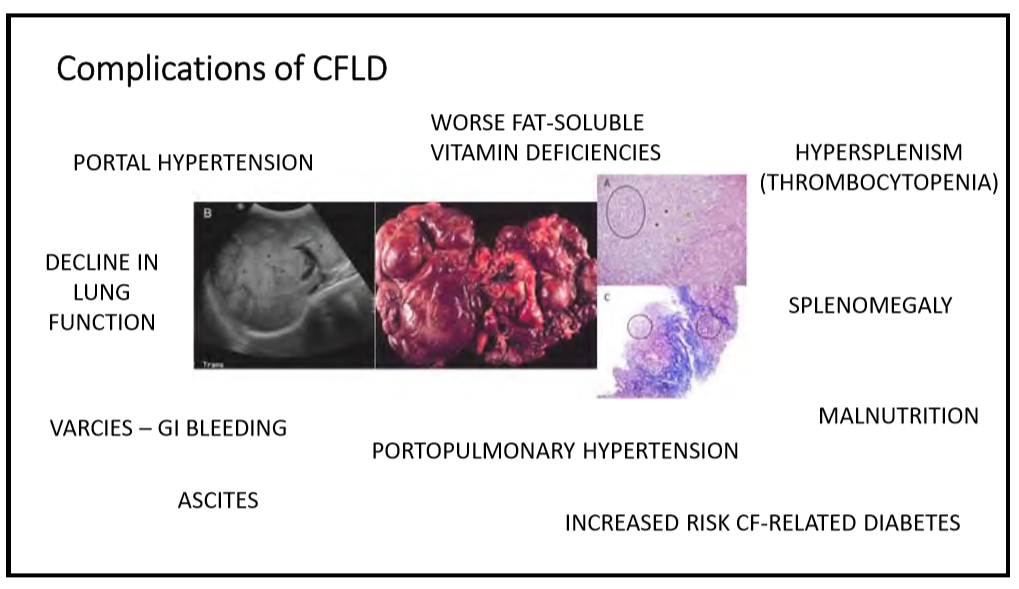
56 Meghana Sathe, MD, UT Southwestern Medical Center The role of the gastroenterologist and hepatologist in Cystic Fibrosis (CF) care today
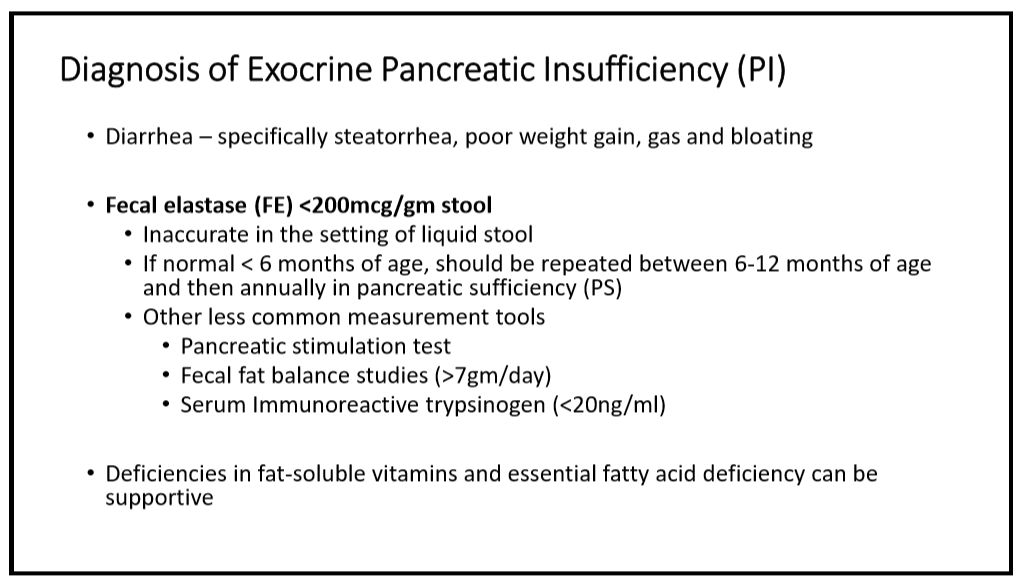
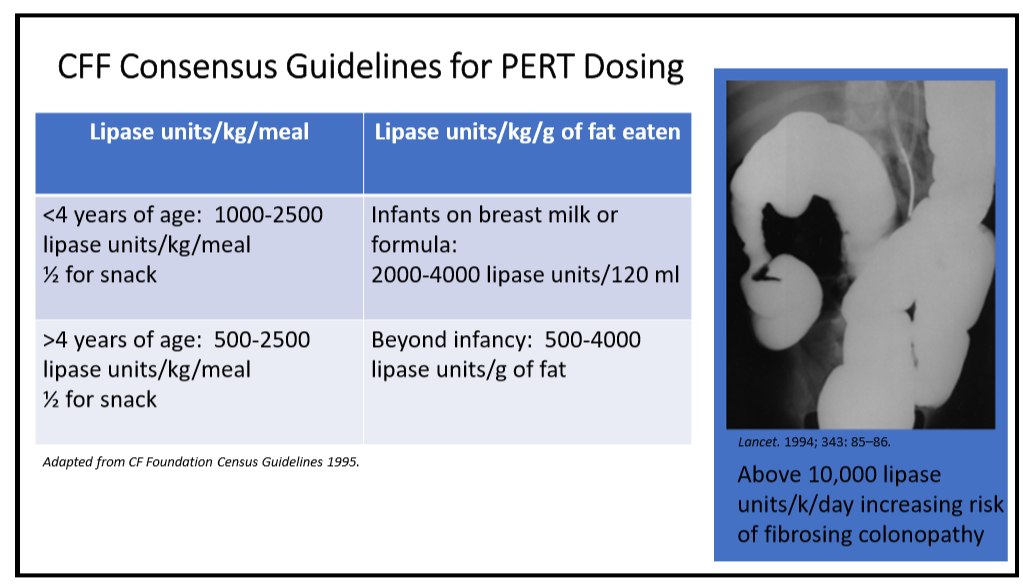
- Fecal elastase monitoring useful for determining need for PERT.
- Discussed CF liver involvement. Multilobular cirrhosis, 7% of individuals, is most important liver disease in CF.
- Modulator therapy can elevate liver enzymes and may need to hold if ALT >5 ULN or lower elevation if elevated bilirubin (see Stop Rules -Practical Advice on DILI)
- DIOS -for partial obstruction, polyethylene glycol and/or gastrogastrin enemas could be used.
- Consider treatment of SBBO as well which is frequent with CF.




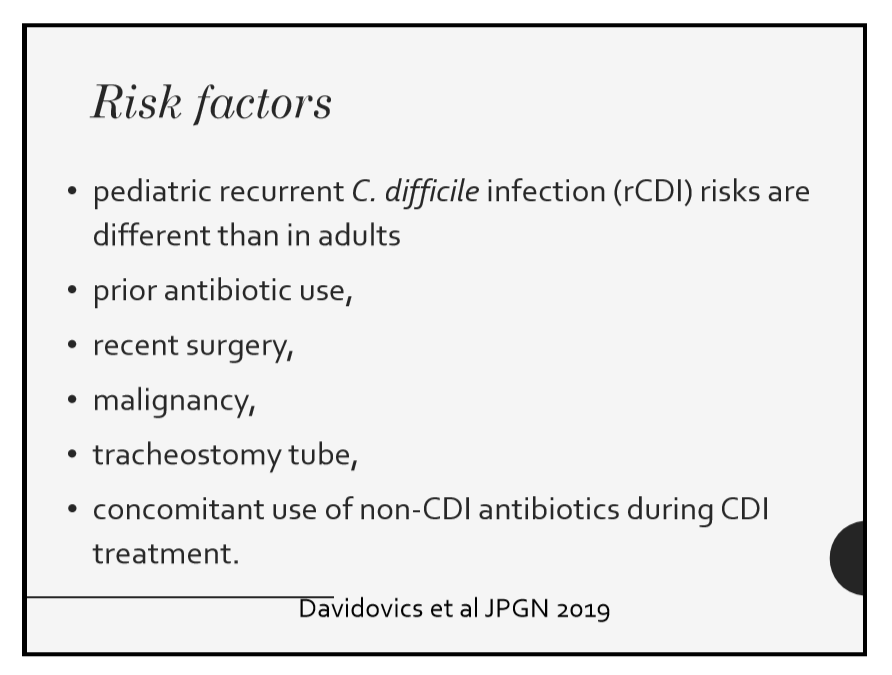
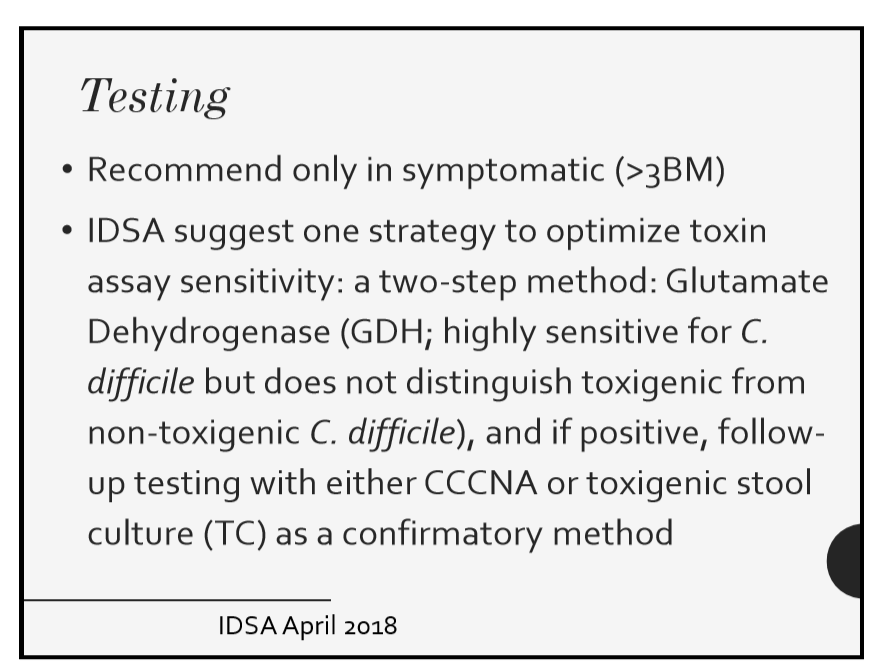
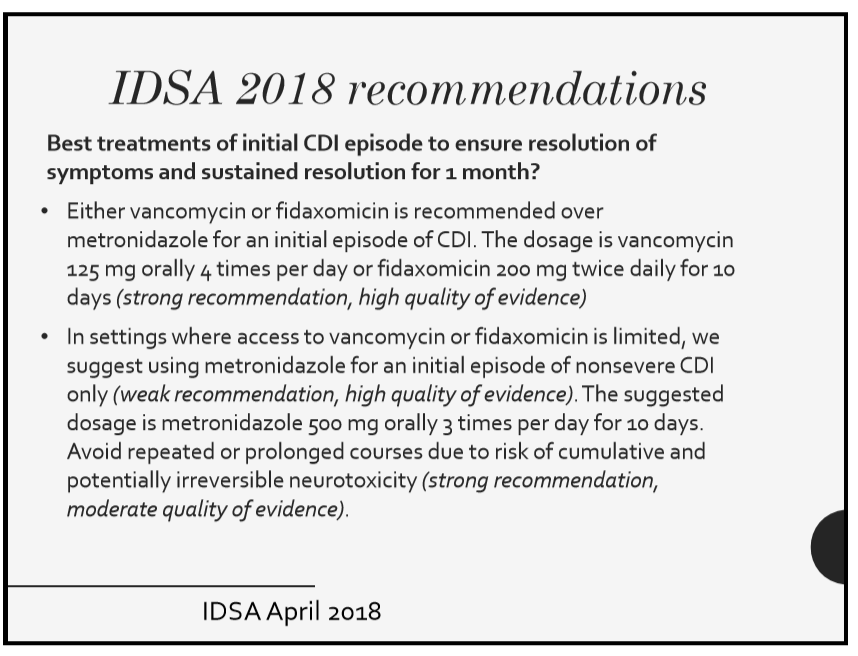
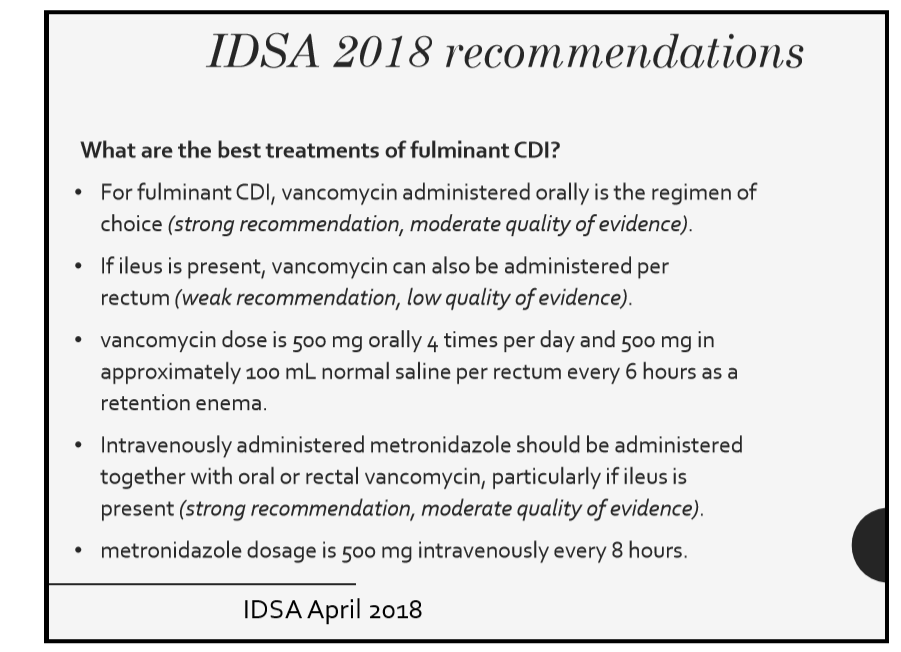
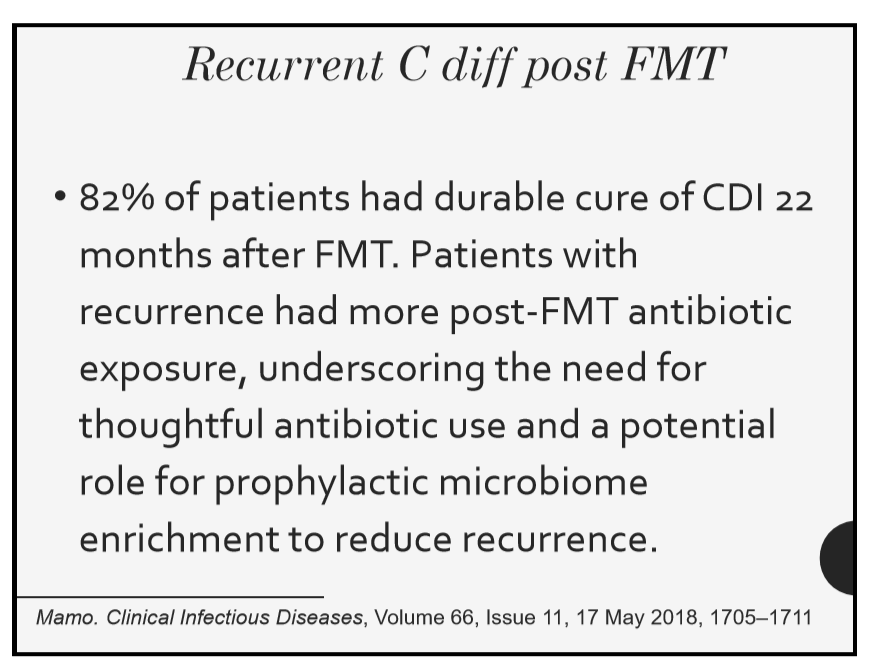
67 Sonia Michail, MD, Children’s Hospital Los Angeles Update on C. difficile
The slide I liked the best was showing a change in microbiome after FMT which is not in syllabus.

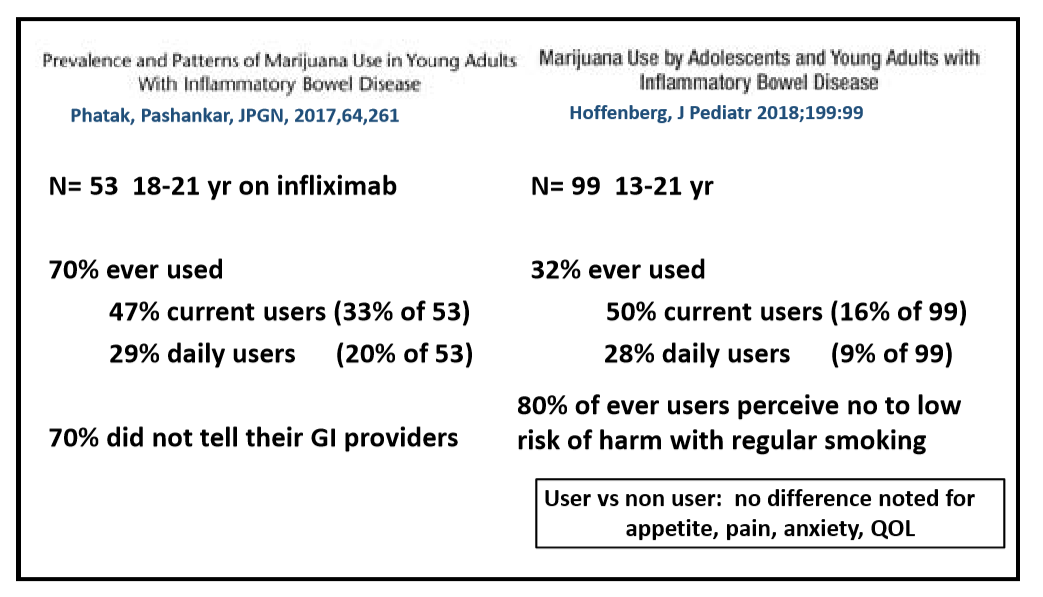
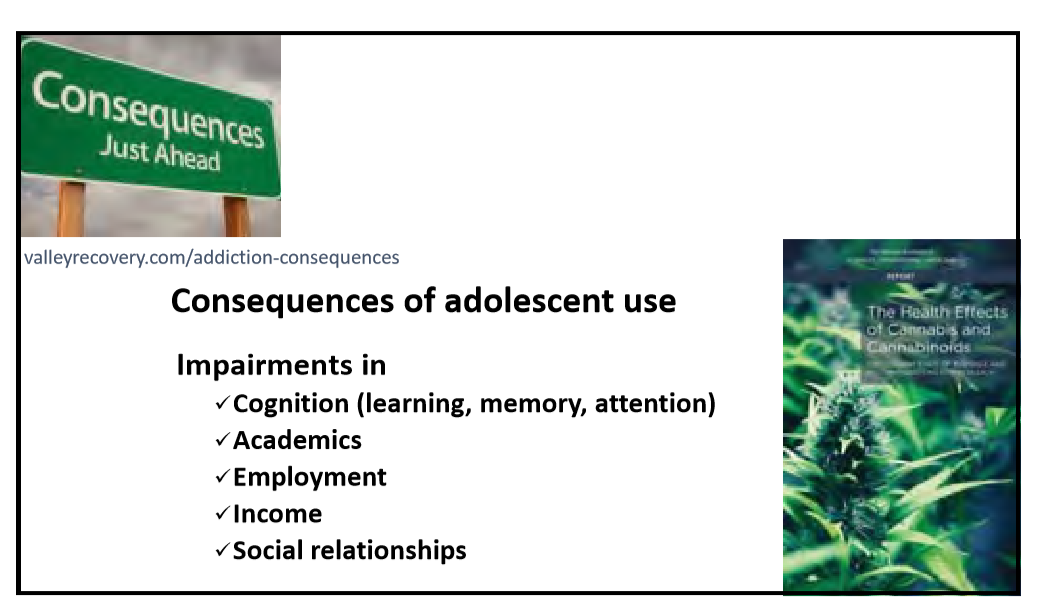
82 Ed Hoffenberg, MD, Children’s Hospital Colorado What the pediatric GI provider needs to know about cannabis



Disclaimer: NASPGHAN/gutsandgrowth assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. The discussion, views, and recommendations as to medical procedures, choice of drugs and drug dosages herein are the sole responsibility of the authors. Because of rapid advances in the medical sciences, the Society cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. Some of the slides reproduced in this syllabus contain animation in the power point version. This cannot be seen in the printed version.

