




Briefly noted: A Muntaner-Mas et al. J Pediatr 2018; 198: 90-7. This cross-sectional study with 250 Spanish children (10-12 year olds) examined obesity measures, physical fitness measures and academic performance. Key finding: “Children considered fit had better academic performance than their unfit peers…the association between body mass index and GPA was mediated by cardiorespiratory fitness and speed-agility.” The design of this study precludes establishing this association as a causal relationship.

Gibbs Gardens
A recent study (thanks to John Pohl for link from twitter feed) (M Totzauer et al. Obesity 2018; https://doi.org/10.1002/oby.22203) indicates that high protein infant formula is associated with an increased risk of obesity.
From Abstract:
Methods
In a multicenter, double‐blind European trial, healthy infants (N = 1,090) were randomly assigned to different protein content formulas (upper [HP] and lower [LP] limits of the European Union regulations in 2001) during the first year; breastfed infants (N = 588) were recruited for reference values.
Weight, height, and triceps and subscapular skinfold (SF) thickness were measured repeatedly (N = 650 at 6 years), and body composition was estimated (Slaughter). The 99th percentile of fat mass index reference data were used to assess excess body fat at 6 years.
Results
At 2 and 6 years, the study observed greater sum of SFs (Δ 2 years: 0.5 mm, P = 0.026, Δ 6 years: 0.6 mm, P = 0.045), fat mass index (Δ 2 years: 0.12 kg/m², P = 0.008, Δ 6 years: 0.15 kg/m², P = 0.011), and fat‐free mass index (Δ 2 years: 0.17 kg/m², P = 0.003, Δ 6 years: 0.18 kg/m², P = 0.010) in the HP group compared with the LP group. At 6 years, the HP group had a twofold higher risk than the LP group for excess body fat (adjusted odds ratio: 2.13, P = 0.019).
Conclusions
Infant formula with HP levels induced greater fat mass in children from 2 to 6 years. Lowering the protein content of infant formula may result in a healthier body composition in early childhood.


Amelia Island -Sunrise
A recent study (AC Skinner et al. Pediatrics 2018; 141: e20173459) examined obesity prevalence data in children 2-19 years of age from a nationally representative sample (n=3340). Specifically, the authors used NHANES data from 1999-2016. Thanks to John Pohl’s twitter feed for pointing out this reference.
PDF Link: Prevalence of Obesity and Severe Obesity in US Children, 1999-2016
This article is packed with data and breaks down obesity in categories: overweight, class I obesity, class II obesity & class III obesity. It provides data based on gender, age, and ethnicity.
The trend in obesity prevalence is best captured in Figure 1.
Among girls:
Among boys:
My take: This article indicates that the prevalence of childhood obesity in the U.S. is not improving and does not appear to have leveled off as has been suggested by some studies.
Related blog posts:

Tanyard Creek Park
A terrific summary of a recent prospective study (RW Taylor et al. NY Times: What Happens When You Let Babies Feed Themselves?
An excerpt:
Baby-led weaning is an approach to feeding that encourages infants to take control of their eating. It’s based on the premise that infants might be better self-regulators of their food consumption..
A recent randomized controlled trial accomplished what previous work could not. Pregnant women in New Zealand were recruited before they gave birth and randomly assigned to one of two groups…
The study found no significant differences in the children’s body mass indexes at 12 or 24 months. Even when researchers restricted the analyses to the most adherent subjects, there were no significant differences over all in B.M.I…
Nonetheless, there might be merit to giving infants more control over their eating: This study found that baby-led weaning resulted in children who were less fussy about what they ate and who seemed to enjoy their food more…
But if we want to find a larger solution to the issues of overweight American children and obesity, it seems we’re going to have to work harder. Babies aren’t going to solve the problem for us.
My take: This study demonstrates the fallacy of the idea that humans naturally self-regulate the right amount of food intake.

A recent ‘clinical quality forum’ sponsored by The Children’s Care Network (TCCN) and Nutrition4Kids featured several good lectures. The symposium was titled “It’s Alimentary.” What follows are my notes –the full lectures from these talks will be available in the coming weeks on the Nutrition4Kids website. My notes may include some errors in transcription and errors of omission.
“The Importance of Intestinal Microbiota in Pediatric Health and Disease” by W Allan Walker (Harvard Medical School, Director of Division of Nutrition) reviewed data showing how changes in the microbiome, likely related to a ‘Western lifestyle’ has resulted in numerous health consequences.
Key points:
Related blog posts:

A subsequent segment addressed “Weight Bias in Healthcare Professionals and What We Can Do About It” by Sheethal Reddy (Strong4Life Clinical Psychologist).
Key points:
Related blog posts:




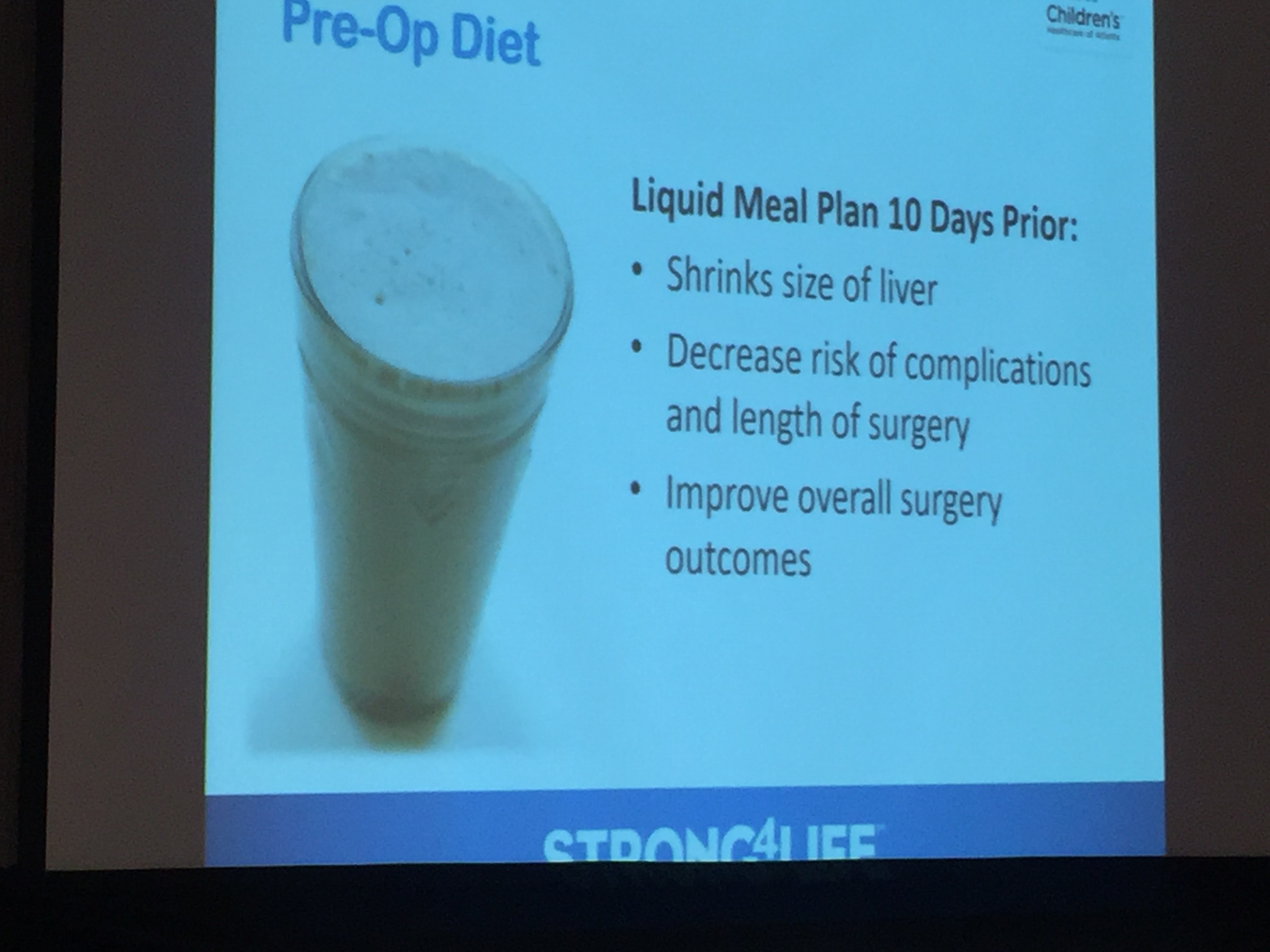
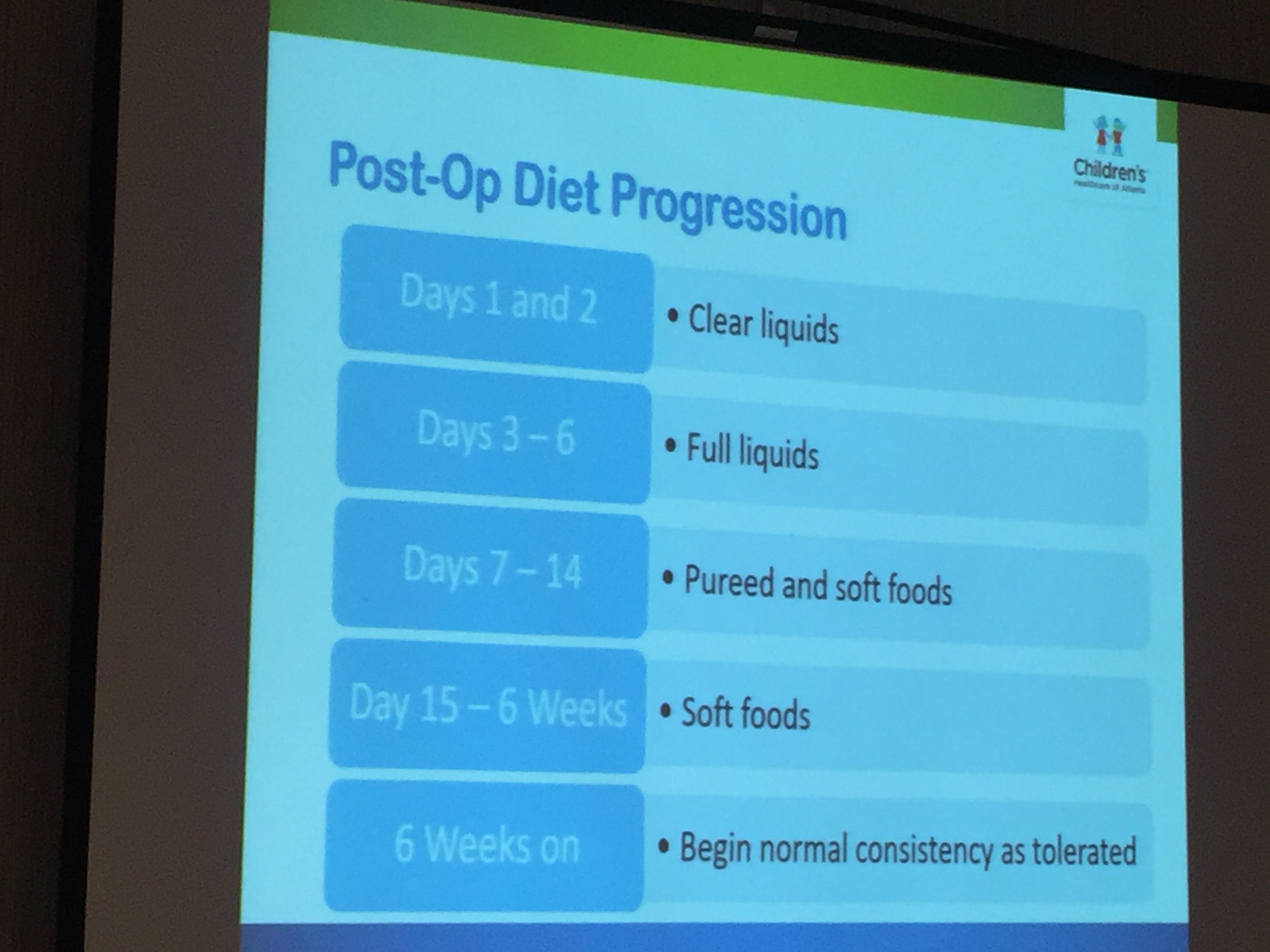
In another talk was related to obesity: “ERAS Nutrition in Bariatric Surgery” by Mark Wulkan (Emory University Professor of Surgery). ERAS is an acronym for Enhanced Recovery After Surgery –pioneered in colorectal surgery (Previous post on ERAS: ERAS-Enhanced Recovery after surgery)
Key points:
Related blog entries:

Bariatric Surgery Candidates




V Shakhnovich et al. J Pediatr 2018; 193: 102-8. Using pharmocokinetic data from 41 obese children (6-17 years), the authors conclude that lean body weight dosing of pantoprazole led to pantoprazole pharmocokinetics similar to nonobese peers. They also note that variability in age-related changes in CYP2C19 activity affected pantoprazole values in children <12 years of age.
Related blog post: #NASPGHAN17 EoE Session -James Franciosis presented data on how CYP2C19*17 allele was important in whether patients responded to PPIs for Eosinophilic Esophagitis.

Bright Angel Trail, Grand Canyon
A recent NY Times article, Do Parents Make Kids Fat, explores the issues of parents being considered responsible for enabling their children to become fat.
Here’s an excerpt:
“When you are the parent of an obese child, there is tremendous stigma,” said Dr. Julie Lumeng, a professor of pediatrics at the University of Michigan. “Everyone looks at the parent and thinks: That parent is incompetent. They don’t care about their child. Why can’t they just make the child eat less and exercise?”
There’s an underlying assumption here about what adults can control, and about how children can be controlled, if only their parents would take the trouble, or make and enforce healthy rules for the whole family, or read the nutritional information on the back of the cereal box….
So yes, for all children, whatever their risk for obesity, good parental decisions about nutrition really matter: It’s important not to overfeed babies, to keep junk food and sugary drinks out of the house, to not let kids eat in front of the screen, and to encourage kids to “eat the rainbow” of fruits and vegetables. But those who rush to judgment should be aware that it is not at all simple to “say no” all the time to an extra-hungry child, or to “feed more vegetables” to the kid who refuses to eat anything green.
Most parents — really — are doing our best, in the complicated food environment in which our children are growing up, with the daily struggles of family life…
“The good parenting that a lot of families exercise when it comes to health,” said Dr. Lumeng, “that may be good enough for a lot of kids, but with some kids with a genetic makeup that predisposes them to obesity, it’s not enough.”
Related blog posts:

Reference: Steinsbekk Silje, Klöckner Christian A., Fildes Alison, Kristoffersen Pernille, Rognsås Stine L., and Wichstrøm Lars. Body Size Estimation from Early to Middle Childhood: Stability of Underestimation, BMI, and Gender Effects. Front. Psychol., 21 November 2017. DOI: 10.3389/fpsyg.2017.02038
This recent study examined how children perceive their own body size. Given the prevalence of overweight/obesity, an accurate understanding of body size is needed if one is going to try to work on this issue.
An excerpt of a summary from Brinkwire: Overweight children more likely to underestimate their body size
The study is based on data from the Norwegian research project Tidlig Trygg i Trondheim, a longitudinal population-based study that looks at the risk and protective factors contributing to children’s psychological and social health…
The children were shown seven pictures of girls and boys with known body mass index and asked which picture looked the most like them. The researchers then calculated the difference in BMI between the figure identified by the children and the children’s own BMI based on measured height and weight…
Generally, the researchers found that children more often underestimated than overestimated the size of their body, although the majority made accurate estimates…
“We also found that the higher the children’s BMI, the more they underestimated their size over time,” Steinsbekk says.
The largest children thus underestimated their body size the most and showed an increased degree of underestimation over time (that is, from 6 to 8 and from 8 to 10 years old).
My take: Given the prevalence of overweight/obese children, this has skewed our perception of what a normal weight should be.
Related blog post: Can parents not know if their child is overweight?

Bright Angel Trail, Grand Canyon

Pont SJ, et al. Pediatrics. 2017. doi: 10.1542/peds.2017-3034. A policy statement from the American Academy of Pediatrics addresses the issue of stigma associated wtih pediatric obesity. This is summarized in the following links:
An excerpt form NY Times piece:
Dr. Pont is one of the lead authors of a new policy statement from the American Academy of Pediatrics titled “Stigma Experienced by Children and Adolescents With Obesity.” The statement, published online Monday in the journal Pediatrics, advises pediatricians to use neutral words like “weight” and “body mass index” rather than terms like “obese” and “fat.” …
In a study published earlier this year in the journal Preventive Medicine, Dr. Puhl and her colleagues looked at the longitudinal effects of teenagers being teased about their weight. The study involved over 1,800 people who had been followed for 15 years and are now in their mid 30s…
“These teasing experiences have long-lasting implications for health and for health behavior.” For women especially, these adolescent experiences of teasing by peers or family members were associated with binge eating, poor body image, obesity, and a higher B.M.I. 15 years later, she said; for men there were some of the same associations, including obesity as adults, if they had been teased by their peers as adolescents…
Weight stigma does exactly the opposite; criticizing and inducing shame only make people feel terrible about themselves, not motivated or capable of making changes…
“Recognize that a child is far more than what their weight is, praise them for all the positives, so when we get to some of the more challenging topics, they can still maintain their self-esteem,”…
The most effective way for parents to help a child is to make healthy changes for the whole family, regardless of shape or size, Dr. Pont said. Try making small changes slowly, like adding one new green vegetable into the family diet, not keeping sugary drinks in the home or walking to school instead of driving.
Related blog posts:

Smoke in Grand Canyon after recent brush fires
